

Cell biology and pathology of podocytes
- PMID: 22054238
- PMCID: PMC3600372
- DOI: 10.1146/annurev-physiol-020911-153238
Cell biology and pathology of podocytes
Abstract
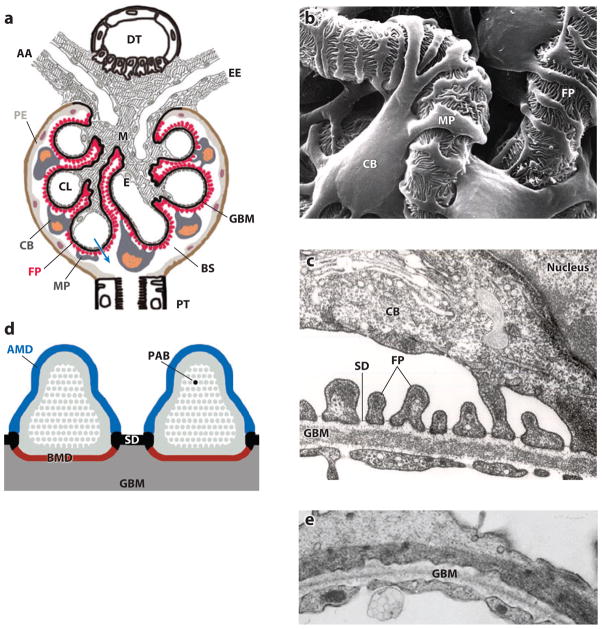
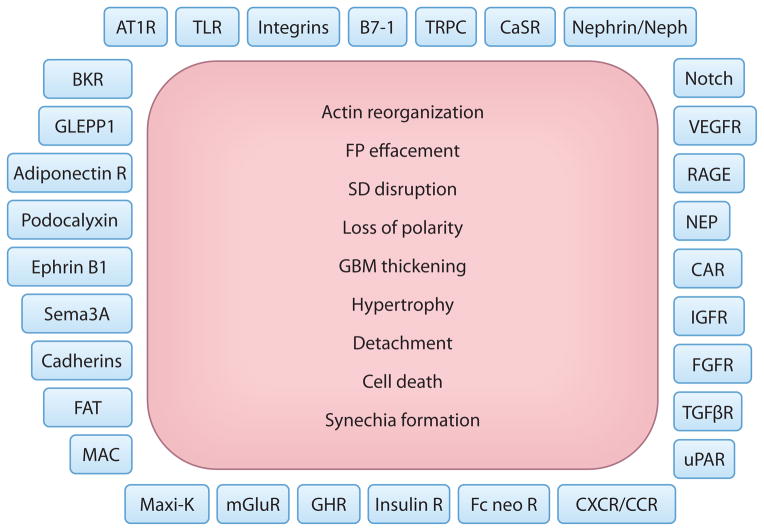
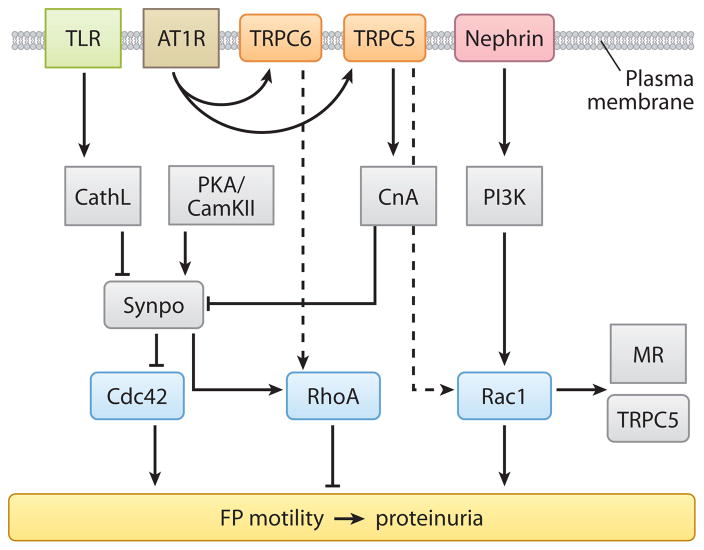
As an integral member of the filtration barrier in the kidney glomerulus, the podocyte is in a unique geographical position: It is exposed to chemical signals from the urinary space (Bowman's capsule), it receives and transmits chemical and mechanical signals to/from the glomerular basement membrane upon which it elaborates, and it receives chemical and mechanical signals from the vascular space with which it also communicates. As with every cell, the ability of the podocyte to receive signals from the surrounding environment and to translate them to the intracellular milieu is dependent largely on molecules residing on the cell membrane. These molecules are the first-line soldiers in the ongoing battle to sense the environment, to respond to friendly signals, and to defend against injurious foes. In this review, we take a membrane biologist's view of the podocyte, examining the many membrane receptors, channels, and other signaling molecules that have been implicated in podocyte biology. Although we attempt to be comprehensive, our goal is not to capture every membrane-mediated pathway but rather to emphasize that this approach may be fruitful in understanding the podocyte and its unique properties.
Figures

References
-
- Mundel P, Kriz W. Structure and function of podocytes: an update. Anat Embryol. 1995;192:385–97. - PubMed
-
- Somlo S, Mundel P. Getting a foothold in nephrotic syndrome. Nat Genet. 2000;24:333–35. - PubMed
-
- Drenckhahn D, Franke RP. Ultrastructural organization of contractile and cytoskeletal proteins in glomerular podocytes of chicken, rat, and man. Lab Investig. 1988;59:673–82. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
