

Identifying patients with suspected gastro-oesophageal cancer in primary care: derivation and validation of an algorithm
- PMID: 22054334
- PMCID: PMC3207088
- DOI: 10.3399/bjgp11X606609
Identifying patients with suspected gastro-oesophageal cancer in primary care: derivation and validation of an algorithm
Abstract
Background: Gastro-oesphageal is one of the most common cancers worldwide. Evidence suggested that increased awareness of symptoms and earlier diagnosis could help improve treatment options and improve survival.
Aim: To derive and validate an algorithm to estimate the absolute risk of having gastro-oesophageal cancer in patients in primary care with and without symptoms.
Design and setting: Cohort study of 375 UK QResearch® general practices for development, and 189 for validation.
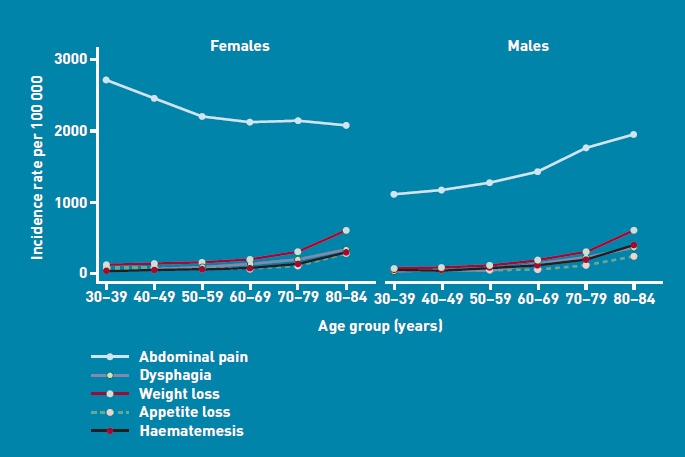
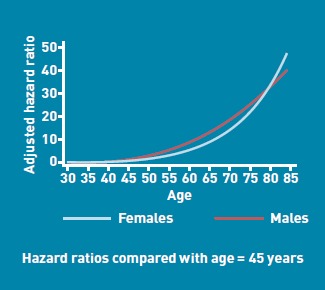
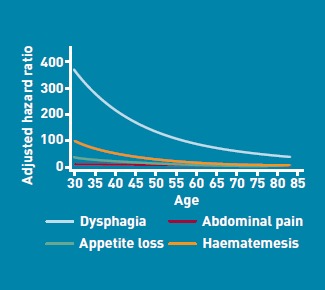
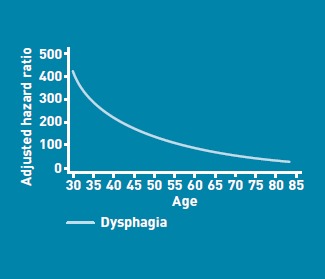
Method: Included patients were aged 30-84 years, free at baseline of a diagnosis of gastro-oesophageal cancer, and without dysphagia, haematemesis, abdominal pain, appetite loss, or weight loss recorded in previous 12 months. The primary outcome was incident diagnosis of gastro-oesophageal cancer recorded in the next 2 years. Risk factors examined were age, body mass index, alcohol status, smoking status, deprivation, family history of gastrointestinal cancer, dysphagia, previous diagnosis of cancer apart from gastro-oesophageal cancer, haematemesis, abdominal pain, appetite loss, weight loss, tiredness, and anaemia. Cox proportional hazards models were used to develop risk equations. Measures of calibration and discrimination assessed performance in the validation cohort.
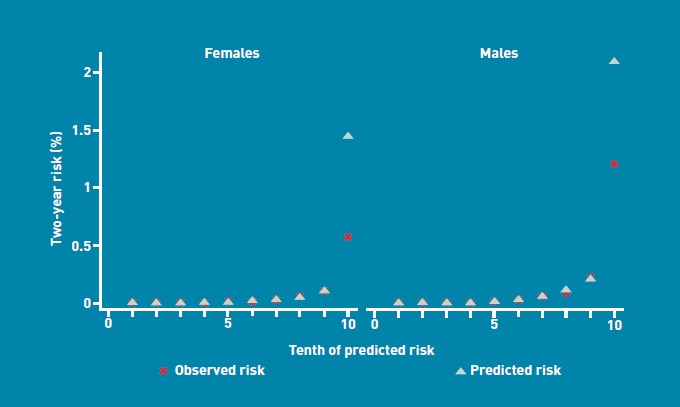
Results: There were 2527 incident cases of gastro-oesophageal cancer from 4.1 million person-years in the derivation cohort. Independent predictors were age, smoking, dysphagia, haematemesis, abdominal pain, appetite loss, weight loss, and anaemia. On validation, the algorithms explained 71% of the variation in females and 73% in males. The receiver operating curve statistics were 0.89 (females) and 0.92 (males). The D statistic was 3.2 (females) and 3.3 (males). The 10% of patients with the highest predicted risks included 77% of all gastro-oesophageal cancers diagnosed over the next 2 years.
Conclusion: The algorithm has good performance and could potentially be used to help identify those at highest risk of gastro-oesophageal cancer, to facilitate early referral and investigation.
Figures
Comment in
-
Cancer and primary care: the clinical and research agenda.Br J Gen Pract. 2011 Nov;61(592):653-4. doi: 10.3399/bjgp11X601523. Br J Gen Pract. 2011. PMID: 22054312 Free PMC article. No abstract available.
-
Predictive effect of heartburn and indigestion and risk of upper gastro-intestinal malignancy.Br J Gen Pract. 2012 Mar;62(596):124-6. doi: 10.3399/bjgp12X629991. Br J Gen Pract. 2012. PMID: 22429415 Free PMC article. No abstract available.
References
-
- Ferlay J, Autier P, Boniol M, et al. Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol. 2007;18(3):581–592. - PubMed
-
- Department of Health. The Cancer Reform Strategy. London: Department of Health; 2007.
-
- Vakil N, Moayyedi P, Fennerty MB, Talley NJ. Limited value of alarm features in the diagnosis of upper gastrointestinal malignancy: systematic review and meta-analysis. Gastroenterology. 2006;131(2):390–401. quiz 659-660. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical