

Progressive induction of left ventricular pressure overload in a large animal model elicits myocardial remodeling and a unique matrix signature
- PMID: 22056365
- PMCID: PMC3241904
- DOI: 10.1016/j.jtcvs.2011.09.032
Progressive induction of left ventricular pressure overload in a large animal model elicits myocardial remodeling and a unique matrix signature
Abstract
Objective: Patients with severe left ventricular pressure overload secondary to aortic stenosis can present with signs and symptoms of heart failure despite normal left ventricular ejection fraction. This process occurs, at least in part, as a result of left ventricular pressure overload-induced extracellular matrix remodeling that promulgates increased left ventricular stiffness and impaired diastolic function. However, the determinants that drive extracellular matrix remodeling in this form of left ventricular pressure overload remain to be fully defined.
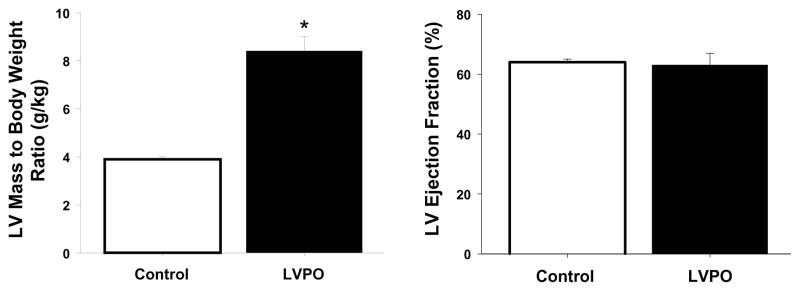
Methods: Left ventricular pressure overload was induced in mature pigs (n = 15) by progressive ascending aortic cuff inflation (once per week for 4 weeks), whereby left ventricular mass, left ventricular ejection fraction, and regional myocardial stiffness (rK(m)) were compared with referent controls (n = 12). Determinants of extracellular matrix remodeling were assessed by measuring levels of mRNA expression for fibrillar collagens, matrix metalloproteinases, and tissue inhibitors of matrix metalloproteinase 1 and 4.
Results: With left ventricular pressure overload, left ventricular mass and rK(m) increased by 2- and 3-fold, respectively, compared with control, with no change in left ventricular ejection fraction. Left ventricular myocardial collagen increased approximately 2-fold, which was accompanied by reduced solubility (ie, increased cross-linking) with left ventricular pressure overload, but mRNA expression for fibrillar collagen and matrix metalloproteinases remained relatively unchanged. In contrast, a robust increase in mRNA expression for tissue inhibitors of matrix metalloproteinase-1 and 4 occurred with left ventricular pressure overload.
Conclusions: In a progressive model of left ventricular pressure overload, which recapitulates the phenotype of aortic stenosis, increased extracellular matrix accumulation and subsequently increased myocardial stiffness were not due to increased fibrillar collagen expression but rather to determinants of post-translational control that included increased collagen stability (thereby resistant to matrix metalloproteinase degradation) and increased endogenous matrix metalloproteinase inhibition. Targeting these extracellular matrix post-translational events with left ventricular pressure overload may hold both diagnostic and therapeutic relevance.
Published by Mosby, Inc.
Figures



References
-
- Monrad ES, Hess OM, Murakami T, et al. Time course of regression of left ventricular hypertrophy after aortic valve replacement. Circulation. 1988;77(6):1345–55. - PubMed
-
- Villari B, Vassalli G, Monrad ES, et al. Normalization of diastolic dysfunction in aortic stenosis late after valve replacement. Circulation. 1995;91:2353–2358. - PubMed
-
- Krayenbuehl HP, Hess OM, Monrad ES, et al. Left ventricular myocardial structure in aortic valve disease before, intermediate, and late after aortic valve replacement. Circulation. 1989;79(4):744–55. - PubMed
-
- Hess OM, Ritter M, Schneider J, et al. Diastolic stiffness and myocardial structure in aortic valve disease before and after valve replacement. Circulation. 1984;69(5):855–65. - PubMed
-
- Azevedo CF, Nigri M, Higuchi ML, et al. Prognostic significance of myocardial fibrosis quantification by histopathology and magnetic resonance imaging in patients with severe aortic valve disease. J Am Coll Cardiol. 2010;56(4):278–87. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
