

Periodontitis and diabetes: a two-way relationship
- PMID: 22057194
- PMCID: PMC3228943
- DOI: 10.1007/s00125-011-2342-y
Periodontitis and diabetes: a two-way relationship
Abstract
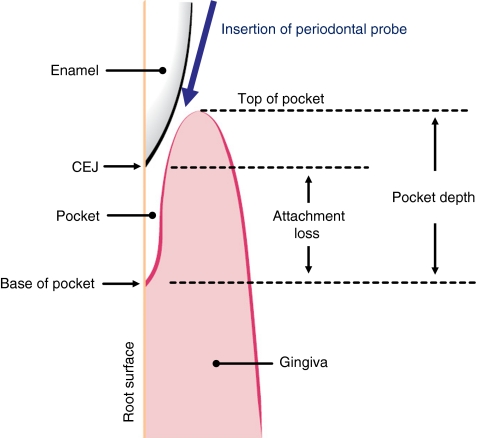
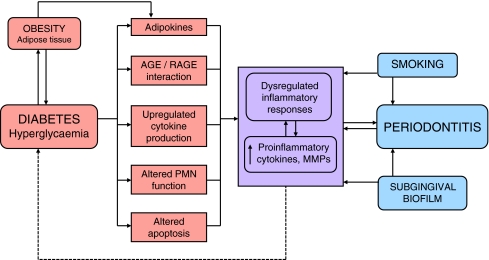
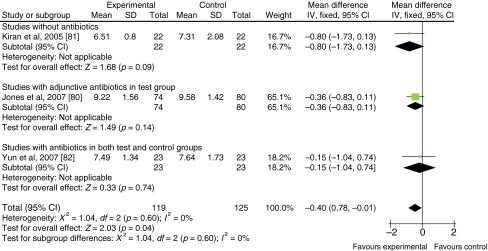
Periodontitis is a common chronic inflammatory disease characterised by destruction of the supporting structures of the teeth (the periodontal ligament and alveolar bone). It is highly prevalent (severe periodontitis affects 10-15% of adults) and has multiple negative impacts on quality of life. Epidemiological data confirm that diabetes is a major risk factor for periodontitis; susceptibility to periodontitis is increased by approximately threefold in people with diabetes. There is a clear relationship between degree of hyperglycaemia and severity of periodontitis. The mechanisms that underpin the links between these two conditions are not completely understood, but involve aspects of immune functioning, neutrophil activity, and cytokine biology. There is emerging evidence to support the existence of a two-way relationship between diabetes and periodontitis, with diabetes increasing the risk for periodontitis, and periodontal inflammation negatively affecting glycaemic control. Incidences of macroalbuminuria and end-stage renal disease are increased twofold and threefold, respectively, in diabetic individuals who also have severe periodontitis compared to diabetic individuals without severe periodontitis. Furthermore, the risk of cardiorenal mortality (ischaemic heart disease and diabetic nephropathy combined) is three times higher in diabetic people with severe periodontitis than in diabetic people without severe periodontitis. Treatment of periodontitis is associated with HbA(1c) reductions of approximately 0.4%. Oral and periodontal health should be promoted as integral components of diabetes management.
Figures

References
-
- Fox CH. New considerations in the prevalence of periodontal disease. Curr Opin Dent. 1992;2:5–11. - PubMed
-
- Fox CH, Jette AM, McGuire SM, Feldman HA, Douglass CW. Periodontal disease among New England elders. J Periodontol. 1994;65:676–684. - PubMed
-
- Kelly M, Steele J, Nuttall N, et al. The condition of supporting structures. In: Walker A, Cooper I, et al., editors. Adult dental health survey: oral health in the United Kingdom 1998. London: The Stationery Office; 2000. pp. 123–146.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
