

The financial impact of health information exchange on emergency department care
- PMID: 22058169
- PMCID: PMC3341788
- DOI: 10.1136/amiajnl-2011-000394
The financial impact of health information exchange on emergency department care
Abstract
Objective: To examine the financial impact health information exchange (HIE) in emergency departments (EDs).
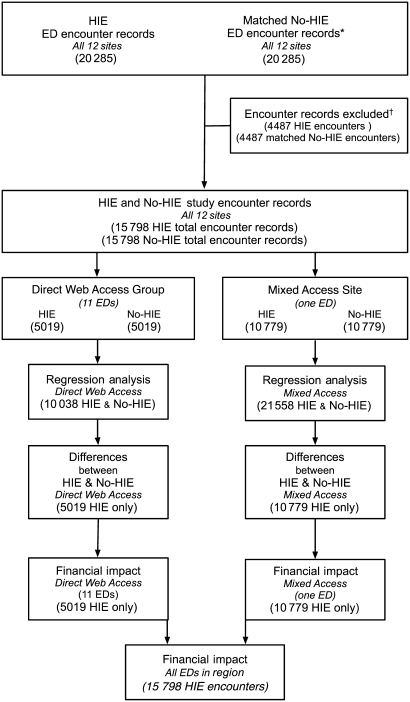
Materials and methods: We studied all ED encounters over a 13-month period in which HIE data were accessed in all major emergency departments Memphis, Tennessee. HIE access encounter records were matched with similar encounter records without HIE access. Outcomes studied were ED-originated hospital admissions, admissions for observation, laboratory testing, head CT, body CT, ankle radiographs, chest radiographs, and echocardiograms. Our estimates employed generalized estimating equations for logistic regression models adjusted for admission type, length of stay, and Charlson co-morbidity index. Marginal probabilities were used to calculate changes in outcome variables and their financial consequences.
Results: HIE data were accessed in approximately 6.8% of ED visits across 12 EDs studied. In 11 EDs directly accessing HIE data only through a secure Web browser, access was associated with a decrease in hospital admissions (adjusted odds ratio (OR)=0.27; p<0001). In a 12th ED relying more on print summaries, HIE access was associated with a decrease in hospital admissions (OR=0.48; p<0001) and statistically significant decreases in head CT use, body CT use, and laboratory test ordering.
Discussion: Applied only to the study population, HIE access was associated with an annual cost savings of $1.9 million. Net of annual operating costs, HIE access reduced overall costs by $1.07 million. Hospital admission reductions accounted for 97.6% of total cost reductions.
Conclusion: Access to additional clinical data through HIE in emergency department settings is associated with net societal saving.
Conflict of interest statement
Figures
References
-
- Burgeois FC, Olson KL, Mandl KD. Patients treated at multiple acute health care facilities: quantifying information fragmentation. Arch Intern Med 2010;170:1989–95 - PubMed
-
- Grumbach K, Bodenheimer T. A primary care home for Americans: putting the house in order. JAMA 2002;288:889–93 - PubMed
-
- Hoffman C, Rice D, Sung HY. Persons with chronic conditions. Their prevalence and costs. JAMA 1996;276:1473–9 - PubMed
-
- Bodenheimer T. Coordinating care – a perilous journey through the health care system. N Engl J Med 2008;358:1064–71 - PubMed
