

Universal antifungal therapy is not needed in persistent febrile neutropenia: a tailored diagnostic and therapeutic approach
- PMID: 22058202
- PMCID: PMC3291604
- DOI: 10.3324/haematol.2011.049999
Universal antifungal therapy is not needed in persistent febrile neutropenia: a tailored diagnostic and therapeutic approach
Abstract
Background: Giving antifungal therapy exclusively to selected patients with persistent febrile neutropenia may avoid over-treatment without increasing mortality. The aim of this study was to validate an innovative diagnostic and therapeutic approach based on assessing patients' risk profile and clinical criteria in order to select those patients requiring antifungal therapy. The efficacy of this approach was compared to that of universal empirical antifungal therapy.
Design and methods: This was a prospective study which included all consecutive adult hematology patients with neutropenia and fever refractory to 5 days of empirical antibacterial therapy admitted to a teaching hospital in Spain over a 2-year period. A diagnostic and therapeutic approach based on clinical criteria and risk profile was applied in order to select patients for antifungal therapy. The sensitivity, specificity and negative predictive value of this approach and also the overall success rate, according to the same criteria of efficacy described in classical clinical trials, were analyzed.
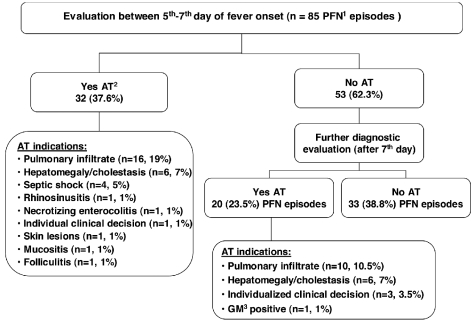
Results: Eighty-five episodes were included, 35 of them (41.2%) in patients at high risk of invasive fungal infections. Antifungal therapy was not indicated in 33 episodes (38.8%). The overall incidence of proven and probable invasive fungal infections was 14.1%, all of which occurred in patients who had received empirical antifungal therapy. The 30-day crude mortality rate was 15.3% and the invasive fungal infection-related mortality rate was 2.8% (2/72). The overall success rate following the diagnostic and therapeutic approach was 36.5% compared with 33.9% and 33.7% obtained in the trial by Walsh et al. The sensitivity, specificity and negative predictive value of the study approach were 100%, 52.4% and 100%, respectively.
Conclusions: Based on the high negative predictive value of this diagnostic and therapeutic approach in persistent febrile neutropenia patients with hematologic malignancies or patients who have received a hematopoietic stem cell transplant, the approach is useful for identifying patients who are not likely to develop invasive fungal infection and do not, therefore, require antifungal therapy. The effectiveness of the strategy is similar to that of universal empirical antifungal therapy reported in controlled trials.
Figures

References
-
- Pagano L, Caira M, Valentini CG, Posteraro B, Fianchi L. Current therapeutic approaches to fungal infections in immunocompromised hematological patients. Blood Rev. 2010;24(2):51–61. - PubMed
-
- Neofytos D, Horn D, Anaissie E, Steinbach W, Olyaei A, Fishman J, et al. Epidemiology and outcome of invasive fungal infection in adult hematopoietic stem cell transplant recipients: analysis of Multicenter Prospective Antifungal Therapy (PATH) Alliance registry. Clin Infect Dis. 2009;48(3):265–73. - PubMed
-
- Pagano L, Girmenia C, Mele L, Ricci P, Tosti ME, Nosari A, et al. Infections caused by filamentous fungi in patients with hematologic malignancies. A report of 391 cases by GIMEMA Infection Program. Haematologica. 2001;86(8):862–70. - PubMed
-
- Pagano L, Caira M, Candoni A, Offidani M, Fianchi L, Martino B, et al. The epidemiology of fungal infections in patients with hematologic malignancies: the SEIFEM-2004 study. Haematologica. 2006;91(8):1068–75. - PubMed
-
- Hughes WT, Armstrong D, Bodey GP, Bow EJ, Brown AE, Calandra T, et al. 2002 guide-lines for the use of antimicrobial agents in neutropenic patients with cancer. Clin Infect Dis. 2002;34(6):730–51. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
