

Clinical approach and treatment of benign and malignant parotid masses, personal experience
- PMID: 22058591
- PMCID: PMC3185824
Clinical approach and treatment of benign and malignant parotid masses, personal experience
Abstract
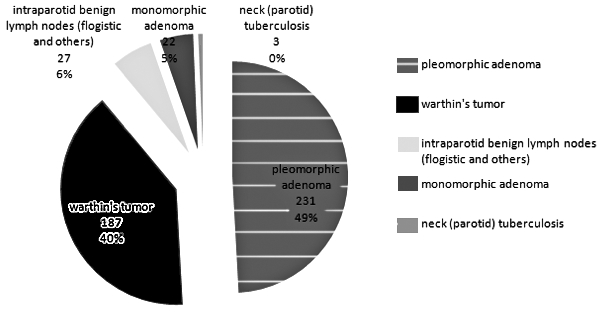
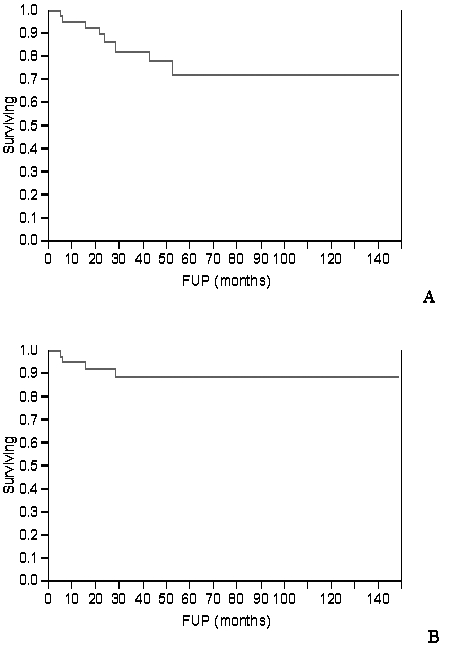
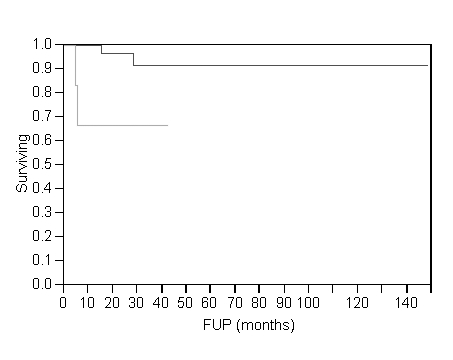
Parotid gland tumours account for 80% of all salivary gland neoplasms, 20% of these are malignant, but in daily clinical practice most parotid masses are operated on before obtaining the final histological diagnosis. This clinical setting further complicates the critical point of parotid surgery, which is the management of the facial nerve. In the present study, data were evaluated referring to 540 patients who underwent parotidectomy for a mass which was discovered to be a benign (470 cases) or a malignant (70 cases) neoplasm, between November 1994 and December 2007, at our Institution. The most significant single parameter in this series of malignancies regarding disease specific survival was the clinical involvement of the facial nerve at diagnosis (p = 0.006). Also for this reason, as there is no evidence that liberal VIIth nerve sacrifice improves prognosis, when it is not clinically involved, every attempt is made to dissect and preserve it. At present, the most complicated situation concerning nerve preservation may be, on the other hand, recurrence of a benign tumour, in particular pleomorphic adenoma, which, in our series, has a higher incidence (8.3%) of permanent facial dysfunction, than surgery with nerve preservation for malignancy (3.7%).
L'80% dei tumori delle ghiandole salivari originano a livello della parotide, il 20% dei tumori parotidei sono maligni. Nella pratica clinica solitamente non è tuttavia possibile stabilire con certezza la diagnosi di natura di una neoformazione parotidea prima della sua asportazione ed esame istologico definitivo. Tale incertezza della diagnosi rende ancora più complicato l'aspetto chiave della chirurgia parotidea, ovvero la gestione del nervo facciale. Abbiamo valutato retrospettivamente 540 pazienti consecutivi sottoposti a parotidectomia presso il nostro reparto di Clinica Otorinolaringoiatrica del Policlinico Gemelli di Roma per una massa della ghiandola, risultata benigna in 470 e maligna in 70 casi, tra il novembre 1994 ed il dicembre 2007. Il singolo parametro clinico più significativo ai fini della prognosi è risultato essere il danno funzionale del nervo facciale alla diagnosi (p = 0,006). Anche per questa ragione, e dal momento che non ci sono prove che il sacrificio sistematico del nervo migliori la prognosi, quando questo non è clinicamente coinvolto, ogni sforzo è effettuato al fine di liberarlo e preservarlo. Particolarmente insidiose da questo punto di vista si sono rivelate le recidive, soprattutto se multifocali, dei tumori benigni, soprattutto degli adenomi pleomorfi. Queste ultime hanno un'incidenza di paresi del facciale permanente post-chirurgica più elevata (8,3%) persino rispetto ai tumori maligni operati con preservazione del nervo (3,7%). In questi casi è fondamentale il consenso del paziente che deve essere adeguatamente informato circa la possibilità di una disfunzione post-chirurgica anche permanente del VII nervo cranico.
Keywords: Facial nerve; Parotid tumours; Prognostic factors.
Figures
References
-
- Spiro R, Spiro J. Cancer of the salivary glands. In: Meyers E, Suen J, editors. Cancer of the head and neck. New York: Churchill Livingstone; 1984. pp. 645–645.
-
- Zbaren P, Schar C, Hotz MA, et al. Value of fine-needle aspiration cytology of parotid gland masses. Laryngoscope. 2001;111:1989–1992. - PubMed
-
- Sergi B, Contucci AM, Corina L, et al. Value of fine-needle aspiration cytology of parotid gland masses. Laryngoscope. 2004;114:789–789. - PubMed
-
- Contucci AM, Corina L, Sergi B, et al. Correlation between fine needle aspiration biopsy and histologic findings in parotid masses. Personal experience. Acta Otorhinolaryngol Ital. 2003;23:314–318. - PubMed
-
- Rea PM, McGarry G, Shaw-Dunn J, et al. The precision of four commonly used surgical landmarks for locating the facial nerve in anterograde parotidectomy in humans. Ann Anat. 2010;192:27–32. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources