

Using Telehealth technology to deliver pulmonary rehabilitation in chronic obstructive pulmonary disease patients
- PMID: 22059179
- PMCID: PMC3205102
- DOI: 10.1155/2011/640865
Using Telehealth technology to deliver pulmonary rehabilitation in chronic obstructive pulmonary disease patients
Abstract
Background: Pulmonary rehabilitation (PR) is an effective therapeutic strategy to improve health outcomes in patients with chronic obstructive pulmonary disease (COPD); however, there is insufficient PR capacity to service all COPD patients, thus necessitating creative solutions to increase the availability of PR.
Objective: To examine the efficacy of PR delivered via Telehealth (Telehealth-PR) compared with PR delivered in person through a standard outpatient hospital-based program (Standard-PR).
Methods: One hundred forty-seven COPD patients participated in an eight-week rural PR program delivered via Telehealth-PR. Data were compared with a parallel group of 262 COPD patients who attended Standard-PR. Education sessions were administered two days per week via Telehealth, and patients exercised at their satellite centre under direct supervision. Standard-PR patients viewed the same education sessions in person and exercised at the main PR site. The primary outcome measure was change in quality of life as evaluated by the St George's Respiratory Questionnaire (SGRQ). A noninferiority analysis was performed using both intention-to-treat and per-protocol approaches.
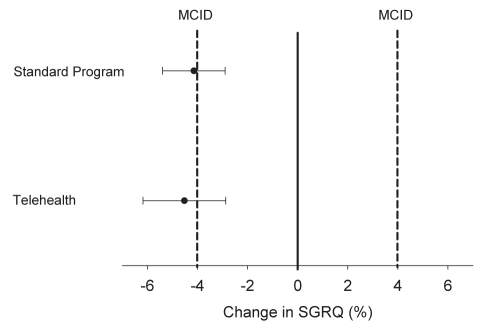
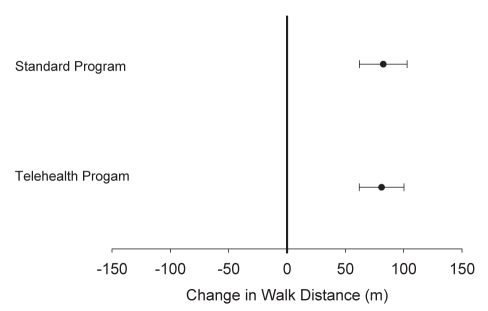
Results: Both Telehealth-PR and Standard-PR resulted in clinically and statistically significant improvements in SGRQ scores (4.5 ± 0.8% versus 4.1 ± 0.6%; P<0.05 versus baseline for both groups), and the improvement in SGRQ was not different between the two programs. Similarly, exercise capacity, as assessed by 12 min walk test, improved equally in both Telehealth-PR and Standard-PR programs (81±10 m versus 82 ± 10 m; P<0.05 versus baseline for both groups).
Conclusion: Telehealth-PR was an effective tool for increasing COPD PR services, and demonstrated improvements in quality of life and exercise capacity comparable with Standard-PR.
HISTORIQUE :: La réadaptation pulmonaire (RP) est une stratégie thérapeutique efficace pour améliorer les issues de santé chez les patients ayant une maladie pulmonaire obstructive chronique (MPOC). Cependant, la capacité de la RP est insuffisante pour servir tous les patients atteints d’une MPOC, ce qui exige des solutions créatives pour accroître la disponibilité de la RP.
OBJECTIF :: Examiner l’efficacité de la RP offerte par télésanté (RP-télésanté) par rapport à la RP offerte en personne au moyen d’un programme ambulatoire en milieu hospitalier (RP-standard).
MÉTHODOLOGIE :: Cent quarante-sept patients atteints de MPOC ont participé à un programme de RP-télésanté de huit semaines en milieu rural. Les chercheurs ont comparé les données avec un groupe parallèle de 262 patients atteints de MPOC qui participaient à une RP-standard. Les séances étaient données deux fois par semaine par télésanté, et les patients s’exerçaient à leur centre satellite sous une supervision directe. Les patients recevant la RP-standard avaient droit aux mêmes séances, en salle, et s’exerçaient à l’établissement principal de la RP. La mesure d’issue primaire était un changement de la qualité de vie évalué par le questionnaire respiratoire de St George (SGRQ). Les chercheurs ont effectué une analyse de non-infériorité au moyen des démarches d’intention de traiter et de respect du protocole.
RÉSULTATS :: Tant la RP-télésanté que la RP-standard ont suscité des améliorations cliniques statistiquement significatives selon les indices de SGRQ (4,5±0,8 % par rapport à 4,1±0,6 %; P<0,05 par rapport aux données de départ dans les deux groupes). Cependant, il n’y avait pas d’amélioration aux indices de SGRQ entre les deux programmes. De même, la capacité à l’exercice, évaluée par un test à l’effort de 12 min, s’est autant améliorée dans le programme de RP-télésanté que dans celui de RP-standard (81±10 m par rapport à 82±10 m; P<0,05 par rapport aux données de départ dans les deux groupes).
CONCLUSION :: La RP-télésanté était un outil efficace pour accroître les services de RP en MPOC et a suscité des améliorations de la qualité de vie et une capacité à l’exercice comparables à la RP-standard.
Figures
Comment in
-
Telehealth technology: an emerging method of delivering pulmonary rehabilitation to patients with chronic obstructive pulmonary disease.Can Respir J. 2011 Jul-Aug;18(4):196. doi: 10.1155/2011/279201. Can Respir J. 2011. PMID: 22059177 Free PMC article. No abstract available.
References
-
- Pulmonary rehabilitation: Joint ACCP/AACVPR evidence-based guidelines ACCP/AACVPR Pulmonary Rehabilitation Guidelines Panel. American College of Chest Physicians. American Association of Cardiovascular and Pulmonary Rehabilitation. Chest. 1997;112:1363–96. - PubMed
-
- Ries AL, Bauldoff GS, Carlin BW, et al. Pulmonary Rehabilitation: Joint ACCP/AACVPR Evidence-Based Clinical Practice Guidelines. Chest. 2007;131:4S–42S. - PubMed
-
- Lacasse Y, Goldstein R, Lasserson TJ, Martin S. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2006:CD003793. - PubMed
-
- Lacasse Y, Wong E, Guyatt GH, King D, Cook DJ, Goldstein RS. Meta-analysis of respiratory rehabilitation in chronic obstructive pulmonary disease. Lancet. 1996;348:1115–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
