

Nonpharmacological management of procedural pain in infants and young children: an abridged Cochrane review
- PMID: 22059204
- PMCID: PMC3206782
- DOI: 10.1155/2011/489286
Nonpharmacological management of procedural pain in infants and young children: an abridged Cochrane review
Abstract
Background: Acute pain and distress during medical procedures are commonplace for young children.
Objective: To assess the efficacy of nonpharmacological interventions for acute procedural pain in children up to three years of age.
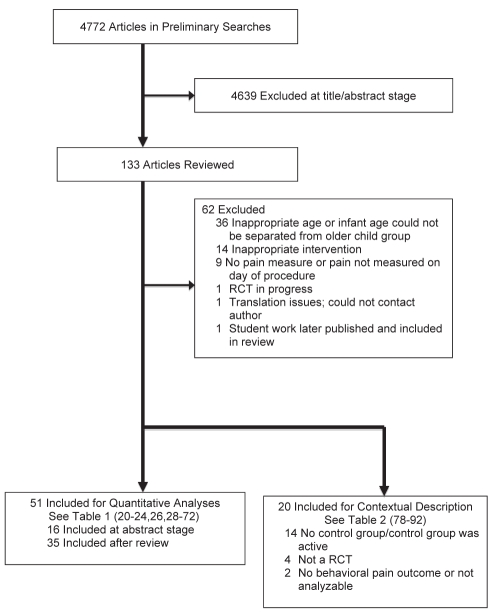
Methods: Study inclusion criteria were: participants <3 years of age, involved in a randomized controlled or crossover trial, and use of a 'no treatment' control group (51 studies; n=3396). Additional studies meeting all criteria except for study design (eg, use of active control group) were qualitatively described (n=20).
Results: For every intervention, data were analyzed separately according to age group (preterm-born, term-born neonate and older infant ⁄ young child) and type of pain response (pain reactivity, immediate pain-related regulation). The largest standardized mean differences (SMD) for pain reactivity were as follows: sucking-related interventions (preterm: -0.42 [95% CI -0.68 to -0.15]; neonate -1.45 [CI -2.34 to -0.57]), kangaroo care (preterm -1.12 [95% CI -2.04 to -0.21]), and swaddling ⁄ facilitated tucking (preterm -0.97 [95% CI -1.63 to -0.31]). For immediate pain-related regulation, the largest SMDs were: sucking-related interventions (preterm -0.38 [95% CI -0.59 to -0.17]; neonate -0.90 [CI -1.54 to -0.25]), kangaroo care 0.77 (95% CI -1.50 to -0.03]), swaddling ⁄ facilitated tucking (preterm -0.75 [95% CI -1.14 to -0.36]), and rocking ⁄ holding (neonate -0.75 [95% CI -1.20 to -0.30]). The presence of significant heterogeneity limited confidence in nonsignificant findings for certain other analyses.
Conclusions: Although a number of nonpharmacological treatments have sufficient evidence supporting their efficacy with preterm infants and healthy neonates, no treatments had sufficient evidence to support efficacy with healthy older infants ⁄ young children.
HISTORIQUE :: Il est courant que les jeunes enfants ressentent une douleur aiguë et de la détresse pendant des interventions médicales.
OBJECTIF :: Évaluer l’efficacité de mesures non pharmacologiques pour sou-lager une douleur aiguë causée par une intervention chez des enfants de moins de trois ans.
MÉTHODOLOGIE :: Les critères d’inclusion dans l’étude s’établissaient comme suit : participants de moins de trois ans faisant partie d’un essai aléatoire et contrôlé ou transversal et utilisation d’un groupe témoin « sans traitement » (51 études; n=3 396). Des études supplémentaires respectant tous les critères sauf la méthodologie (p. ex., recours à un groupe témoin actif) ont fait l’objet d’une description qualitative (n=20).
RÉSULTATS :: À chaque intervention, les chercheurs ont analysé les données séparément compte tenu du groupe d’âge (nouveau-né prématuré ou à terme et nourrisson plus âgé ou jeune enfant) et du type de réponse à la douleur (réactivité à la douleur, régulation immédiate liée à la douleur). Les plus grandes différences moyennes standardisées (DMS) de réactivité à la douleur s’établissaient comme suit : interventions liées à la succion (prématuré : −0,42 [95 % IC −0,68 à −0,15]; nouveau-né : −1,45 [IC −2,34 à −0,57]), technique kangourou (prématuré : −1,12 [95 % IC −2,04 à −0,21]) et emmaillotement ou enroulement facilité (prématuré : −0,97 [95 % IC −1,63 à −0,31]). En cas de régulation immédiate liée à la douleur, les plus grandes DMS s’établissaient comme suit : interventions liées à la succion (prématuré : −0,38 [95 % IC −0,59 à −0,17]; nouveau-né : −0,90 [IC −1,54 à −0,25]), technique kangourou : 0,77 (95 % IC −1,50 à −0,03]), emmaillotement ou enroulement facilité (prématuré : −0,75 [95 % IC −1,14 à −0,36]), et fait de bercer ou de prendre dans les bras (nouveau-né : −0,75 [95 %IC −1,20 à −0,30]). Une hétérogénéité importante limitait l’intervalle de confiance des résultats non significatifs de certaines autres analyses.
CONCLUSIONS :: Même si les données sont suffisantes pour appuyer l’efficacité d’un certain nombre de traitements chez les prématurés et les nouveau-nés en santé, aucun traitement ne s’associe à des données probantes suffisantes pour en étayer l’efficacité chez les nourrissons plus âgés et les jeunes enfants.
Figures
Comment in
-
Pain control in infants and young children.Pain Res Manag. 2011 Sep-Oct;16(5):320. doi: 10.1155/2011/505039. Pain Res Manag. 2011. PMID: 22059203 Free PMC article. No abstract available.
References
-
- Field T. Infancy is not without pain. Vasta R, editor. Annals of Child Development: A research annual. 1995;10:1–26.
-
- Johnston CC, Stevens B, Craig KD, Grunau RV. Developmental changes in pain expression in premature, full-term, two and four-month-old infants. Pain. 1993;52:201–208. - PubMed
-
- Berde CB, Jaksic T, Lynn AM, Maxwell LG, Soriano SG, Tibboel D. Anaesthesia and analgesia during and after surgery in neonates. Clin Ther. 2005;27:900–21. - PubMed
-
- Fitzgerald M. The development of nociceptive circuits. Nat Rev Neurosci. 2005;6:507–20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
