

Concurrent temozolomide and dose-escalated intensity-modulated radiation therapy in newly diagnosed glioblastoma
- PMID: 22065084
- PMCID: PMC3266840
- DOI: 10.1158/1078-0432.CCR-11-2073
Concurrent temozolomide and dose-escalated intensity-modulated radiation therapy in newly diagnosed glioblastoma
Abstract
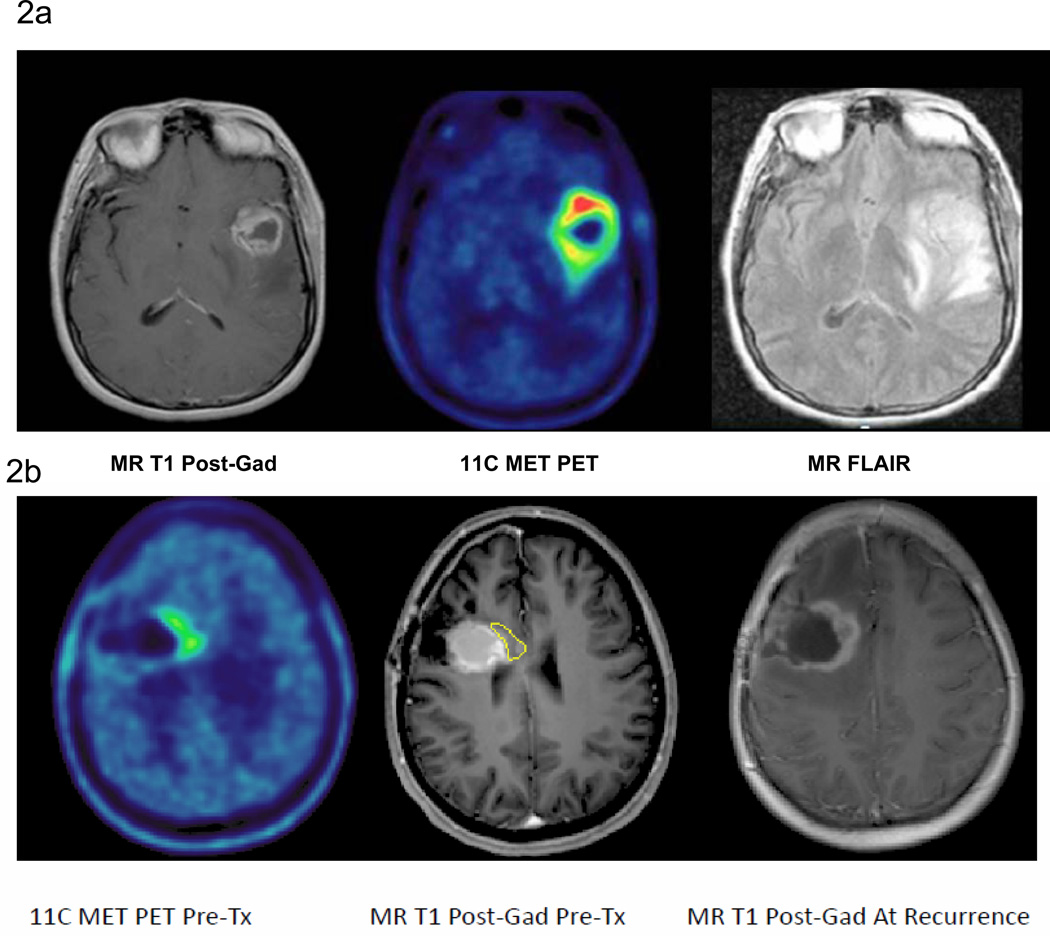
Purpose: To determine the maximum-tolerated dose (MTD) of radiation (RT) with concurrent temozolomide in patients with newly diagnosed glioblastoma (GBM), to estimate their progression-free (PFS) and overall survival (OS), and to assess the role of (11)C methionine PET (MET-PET) imaging in predicting recurrence.
Experimental design: Intensity-modulated RT (IMRT) doses of 66 to 81 Gy, assigned to patients by the time-to-event continual reassessment method, were delivered over 6 weeks with concurrent daily temozolomide (75 mg/m(2)) followed by adjuvant cyclic temozolomide (200 mg/m(2) d1-5 q28d ×6 cycles). Treatment was based on gadolinium-enhanced MRI. Pretreatment MET-PET scans were obtained for correlation with eventual sites of failure.
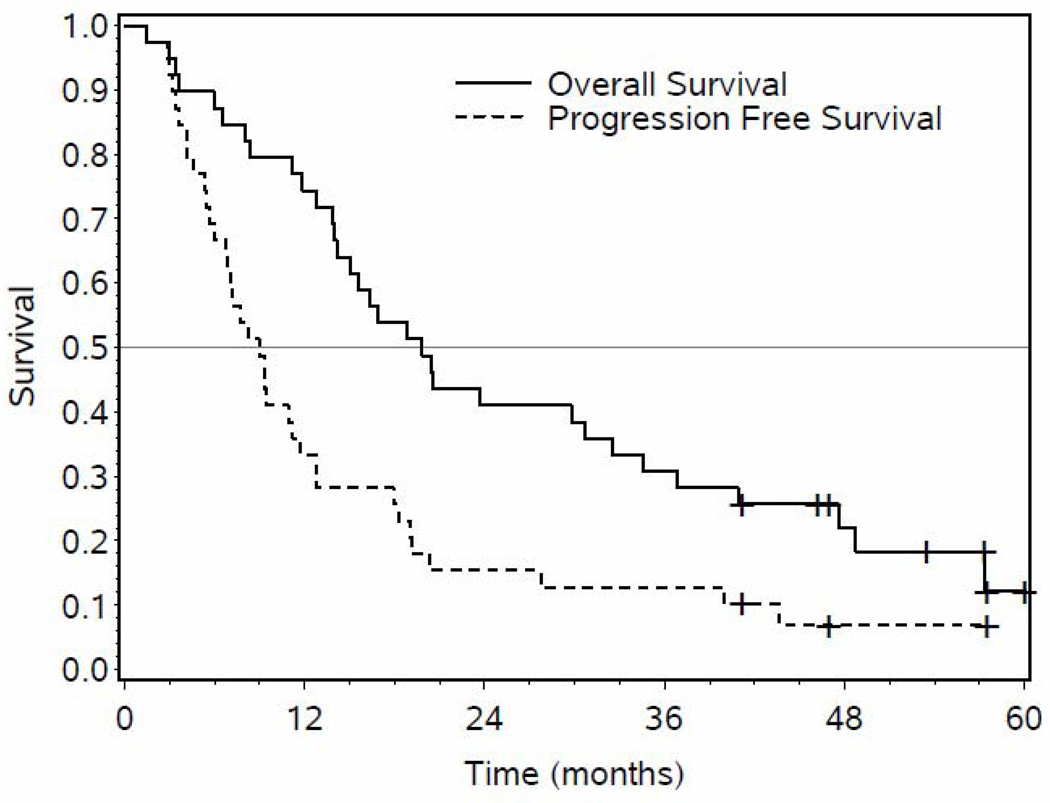
Results: A total of 38 patients were analyzed with a median follow-up of 54 months for patients who remain alive. Late CNS grade ≥III toxicity was observed at 78 (2 of 7 patients) and 81 Gy (1 of 9 patients). None of 22 patients receiving 75 or less Gy developed RT necrosis. Median OS and PFS were 20.1 (14.0-32.5) and 9.0 (6.0-11.7) months, respectively. Twenty-two of 32 patients with pretreatment MET-PET uptake showed uptake beyond the contrast-enhanced MRI. Patients whose treatment did not include the region of increased MET-PET uptake showed an increased risk of noncentral failure (P < 0.001).
Conclusions: Patients with GBM can safely receive standard temozolomide with 75 Gy in 30 fractions, delivered using IMRT. The median OS of 20.1 months is promising. Furthermore, MET-PET appears to predict regions of high risk of recurrence not defined by MRI, suggesting that further improvements may be possible by targeting metabolically active regions.
© 2011 AACR.
Figures
References
-
- Wallner KE, Galicich JH, et al. Patterns of failure following treatment for glioblastoma multiforme and anaplastic astrocytoma. International journal of radiation oncology, biology, physics. 1989;16(6):1405–1409. - PubMed
-
- Garden AS, Maor MH, Yung WK, et al. Outcome and patterns of failure following limited-volume irradiation for malignant astrocytoma. Radiother Oncol. 1991;20(2):99–110. - PubMed
-
- Lee SW, Fraass BA, et al. Patterns of failure following high-dose 3-D conformal RT for high-grade astrocytomas: a quantitative dosimetric study. International journal of radiation oncology, biology, physics. 1999;43(1):79–88. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant TMZ for glioblastoma. N Engl J Med. 2005;352:987–996. - PubMed
-
- Stupp R, Hegi M, et al. Effects of RT with concomitant and adjuvant temozolomide versus RT alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet oncology. 2009;10(5):459–466. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
