

RAS mutations are associated with the development of cutaneous squamous cell tumors in patients treated with RAF inhibitors
- PMID: 22067401
- PMCID: PMC3269955
- DOI: 10.1200/JCO.2011.36.7680
RAS mutations are associated with the development of cutaneous squamous cell tumors in patients treated with RAF inhibitors
Abstract
Purpose: RAF inhibitors are effective against melanomas with BRAF V600E mutations but may induce keratoacanthomas (KAs) and cutaneous squamous cell carcinomas (cSCCs). The potential of these agents to promote secondary malignancies is concerning. We analyzed cSCC and KA lesions for genetic mutations in an attempt to identify an underlying mechanism for their formation.
Methods: Four international centers contributed 237 KA or cSCC tumor samples from patients receiving an RAF inhibitor (either vemurafenib or sorafenib; n = 19) or immunosuppression therapy (n = 53) or tumors that developed spontaneously (n = 165). Each sample was profiled for 396 known somatic mutations across 33 cancer-related genes by using a mass spectrometric-based genotyping platform.
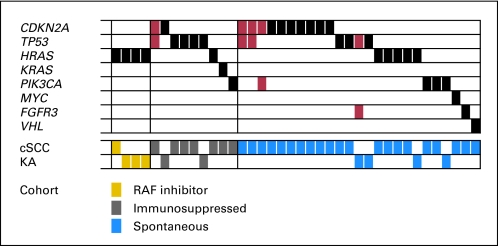
Results: Mutations were detected in 16% of tumors (38 of 237), with five tumors harboring two mutations. Mutations in TP53, CDKN2A, HRAS, KRAS, and PIK3CA were previously described in squamous cell tumors. Mutations in MYC, FGFR3, and VHL were identified for the first time. A higher frequency of activating RAS mutations was found in tumors from patients treated with an RAF inhibitor versus populations treated with a non-RAF inhibitor (21.1% v 3.2%; P < .01), although overall mutation rates between treatment groups were similar (RAF inhibitor, 21.1%; immunosuppression, 18.9%; and spontaneous, 17.6%; P = not significant). Tumor histology (KA v cSCC), tumor site (head and neck v other), patient age (≤ 70 v > 70 years), and sex had no significant impact on mutation rate or type.
Conclusion: Squamous cell tumors from patients treated with an RAF inhibitor have a distinct mutational profile that supports a mechanism of therapy-induced tumorigenesis in RAS-primed cells. Conceivably, cotargeting of MEK together with RAF may reduce or prevent formation of these tumors.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Induction of cutaneous squamous cell carcinomas by RAF inhibitors: cause for concern?J Clin Oncol. 2012 Jan 20;30(3):329-30. doi: 10.1200/JCO.2011.38.2895. Epub 2011 Nov 7. J Clin Oncol. 2012. PMID: 22067405 No abstract available.
Similar articles
-
RAS mutations in cutaneous squamous-cell carcinomas in patients treated with BRAF inhibitors.N Engl J Med. 2012 Jan 19;366(3):207-15. doi: 10.1056/NEJMoa1105358. N Engl J Med. 2012. PMID: 22256804 Free PMC article. Clinical Trial.
-
Inactivation of TGFβ receptors in stem cells drives cutaneous squamous cell carcinoma.Nat Commun. 2016 Aug 25;7:12493. doi: 10.1038/ncomms12493. Nat Commun. 2016. PMID: 27558455 Free PMC article.
-
Skin tumors induced by sorafenib; paradoxic RAS-RAF pathway activation and oncogenic mutations of HRAS, TP53, and TGFBR1.Clin Cancer Res. 2012 Jan 1;18(1):263-72. doi: 10.1158/1078-0432.CCR-11-1344. Epub 2011 Nov 17. Clin Cancer Res. 2012. PMID: 22096025
-
Vemurafenib-induced progression of breast cancer: a case report and review of the literature.Target Oncol. 2016 Apr;11(2):235-8. doi: 10.1007/s11523-015-0384-7. Target Oncol. 2016. PMID: 26264150 Review.
-
[Cellular and molecular mechanisms of carcinogenic side effects and resistance to BRAF inhibitors in metastatic melanoma with BRAFV600 mutation: state of the knowledge].Ann Pathol. 2013 Dec;33(6):375-85. doi: 10.1016/j.annpat.2013.09.003. Epub 2013 Oct 31. Ann Pathol. 2013. PMID: 24331719 Review. French.
Cited by
-
NRAS mutant melanoma: biological behavior and future strategies for therapeutic management.Oncogene. 2013 Jun 20;32(25):3009-18. doi: 10.1038/onc.2012.453. Epub 2012 Oct 15. Oncogene. 2013. PMID: 23069660 Free PMC article. Review.
-
Multiple Gastrointestinal Polyps in Patients Treated with BRAF Inhibitors.Clin Cancer Res. 2015 Dec 1;21(23):5215-21. doi: 10.1158/1078-0432.CCR-15-0469. Epub 2015 Jul 22. Clin Cancer Res. 2015. PMID: 26202952 Free PMC article.
-
MEK Is a Therapeutic and Chemopreventative Target in Squamous Cell Carcinoma.J Invest Dermatol. 2016 Sep;136(9):1920-1924. doi: 10.1016/j.jid.2016.05.110. Epub 2016 Jun 9. J Invest Dermatol. 2016. PMID: 27293029 Free PMC article. No abstract available.
-
Vemurafenib plus cobimetinib in the treatment of mutated metastatic melanoma: the CoBRIM trial.Melanoma Manag. 2015 Aug;2(3):209-215. doi: 10.2217/mmt.15.22. Epub 2015 Aug 10. Melanoma Manag. 2015. PMID: 30190850 Free PMC article. Review.
-
Loss of Tpl2 activates compensatory signaling and resistance to EGFR/MET dual inhibition in v-RAS transduced keratinocytes.PLoS One. 2022 Mar 24;17(3):e0266017. doi: 10.1371/journal.pone.0266017. eCollection 2022. PLoS One. 2022. PMID: 35325006 Free PMC article.
References
-
- Kefford R, Arkenau H, Brown MP, et al. Phase I/II study of GSK2118436, a selective inhibitor of oncogenic mutant BRAF kinase, in patients with metastatic melanoma and other solid tumors. J Clin Oncol. 2010;28(suppl; abst 8503):611s.
-
- Ribas A, Kim KB, Schuchter LM, et al. BRIM-2: An open-label, multicenter phase II study of vemurafenib in previously treated patients with BRAF V600E mutation-positive metastatic melanoma. J Clin Oncol. 2011;29(suppl; abst 8509):528s.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
