

Outcomes of antiretroviral treatment programs in rural Southern Africa
- PMID: 22067665
- PMCID: PMC3259205
- DOI: 10.1097/QAI.0b013e31823edb6a
Outcomes of antiretroviral treatment programs in rural Southern Africa
Abstract
Background: Data on outcomes of antiretroviral treatment (ART) programs in rural sub-Saharan African are scarce. We describe early losses and long-term outcomes in 6 rural programs in Southern Africa with limited access to viral load monitoring and second-line ART.
Methods: Patients aged ≥16 years starting ART in 2 programs each in Zimbabwe, Mozambique, and Lesotho were included. We evaluated risk factors for no follow-up after starting ART and mortality and loss to follow-up (LTFU) over 3 years of ART, using logistic regression and competing risk models. Odds ratios and subdistribution hazard ratios, adjusted for gender, age category, CD4 category, and World Health Organization stage at start of ART are reported.
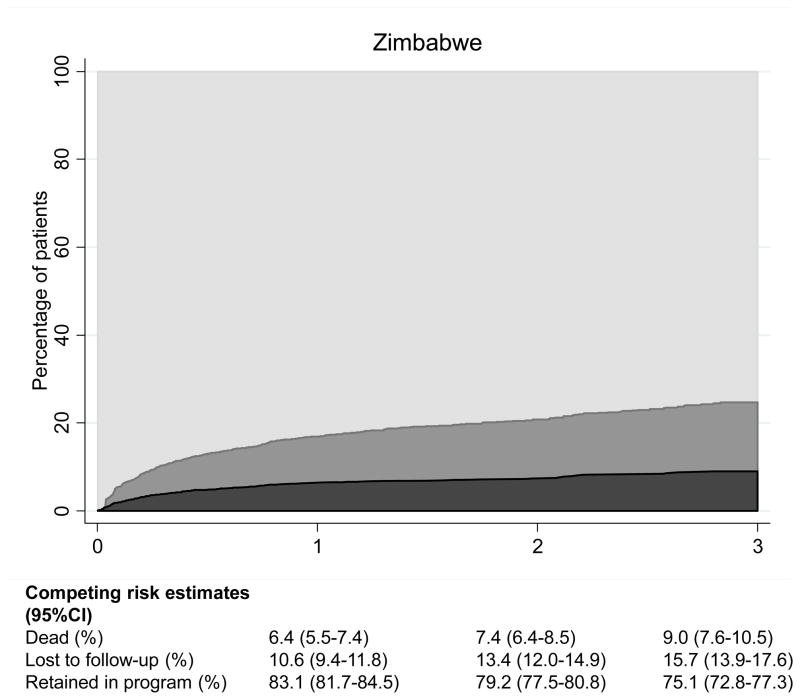
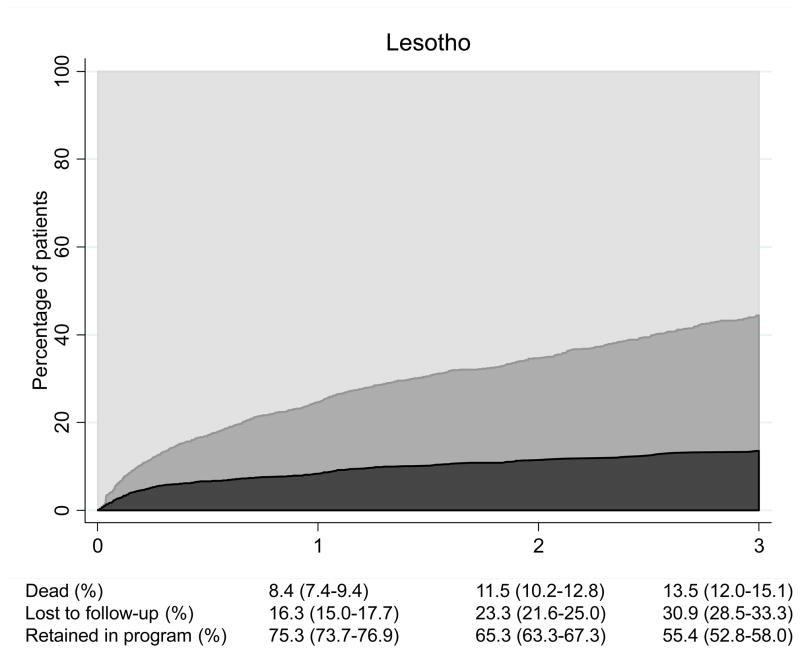
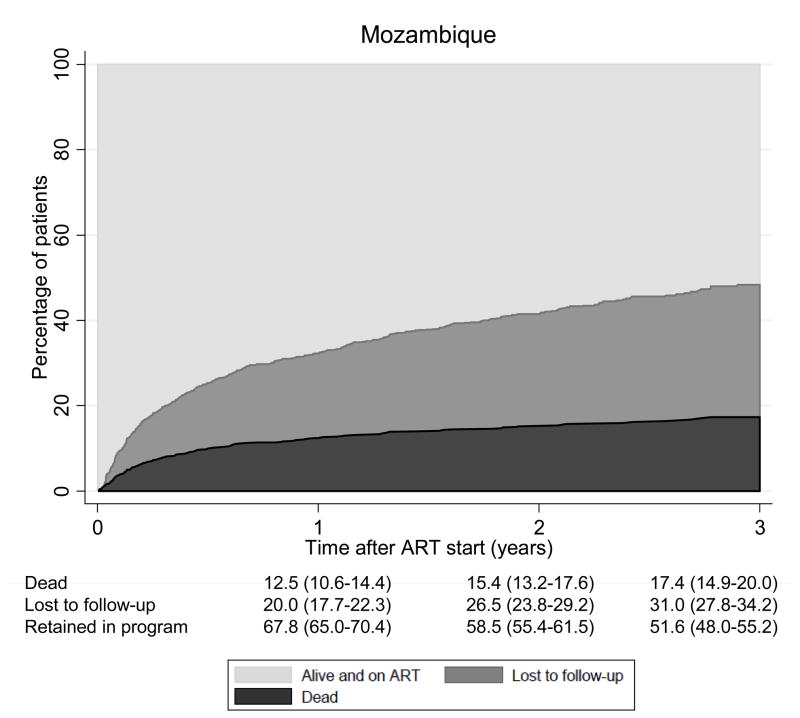
Results: Among 7725 patients, 449 (5.8%) did not return after initiation of ART. During 9575 person-years, 698 (9.6%) of those with at least 1 follow-up visit died, and 1319 (18.1%) were LTFU. At 3 years, the cumulative incidence of death and LTFU were 12.5% (11.5%-13.5%) and 25.4% (24.0%-26.9%), respectively, with important differences between countries as follows: in Zimbabwe 75.1% (72.8%-77.3%) were alive and on ART at 3 years compared with 55.4% (52.8%-58.0%) in Lesotho and 51.6% (48.0%-55.2%) in Mozambique. In all settings, young age and male gender predicted LTFU, whereas advanced clinical stage and low baseline CD4 counts predicted death.
Conclusions: In African ART programs with limited access to second-line treatment, mortality, and LTFU are high in the first 3 years of ART. Low retention in care is a major threat to the sustainability of ART delivery in Southern Africa, particularly in rural sites.
Conflict of interest statement
References
-
- World Health Organization. Progress Report 2010. Geneva, Switzerland: World Health Organization; 2010. Towards Universal Access. Scaling Up Priority HIV/AIDS Interventions in the Health Sector.
-
- Mills EJ, Nachega JB, Buchan I, et al. Adherence to antiretroviral therapy in sub-Saharan Africa and North America: a meta-analysis. JAMA. 2006 Aug 9;296(6):679–690. - PubMed
-
- Nachega JB, Mills EJ, Schechter M. Antiretroviral therapy adherence and retention in care in middle-income and low-income countries: current status of knowledge and research priorities. Curr Opin HIV AIDS. 2010 Jan;5(1):70–77. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
