

Effect of hysterectomy with ovarian preservation on ovarian function
- PMID: 22067716
- PMCID: PMC3223258
- DOI: 10.1097/AOG.0b013e318236fd12
Effect of hysterectomy with ovarian preservation on ovarian function
Abstract
Objective: To prospectively estimate the risk for earlier ovarian failure among women undergoing hysterectomy with ovarian preservation, as compared with women of similar age without hysterectomy.
Methods: A prospective cohort study was conducted among women aged 30 to 47 years undergoing hysterectomy without bilateral oophorectomy (n=406) and women with intact uteri (n=465). Blood samples and questionnaire data were obtained at baseline and annually for up to 5 years. Hazard ratios (HR) for ovarian failure, defined as follicle-stimulating hormone levels 40 international units/L or higher, were calculated using Cox proportional hazards models.
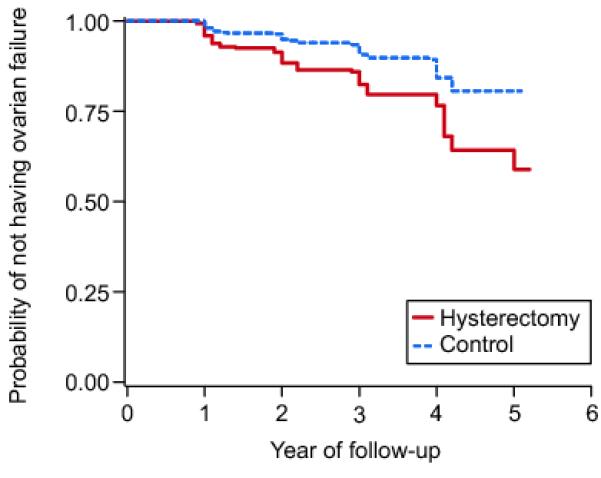
Results: Ovarian failure occurred among 60 of the women with hysterectomy and 46 of the women in the control group. Women undergoing hysterectomy were at nearly a twofold increased risk for ovarian failure as compared with women with intact uteri (HR 1.92, 95% confidence interval [CI] 1.29-2.86). The proportional hazards model further estimated that 14.8% of women with hysterectomies experienced ovarian failure after 4 years of follow-up compared with 8.0% of the women in the control group. Risk for ovarian failure was greater for women who had a unilateral oophorectomy along with their hysterectomy (HR 2.93, 95% CI 1.57-5.49), but also it was significantly increased for women who retained both ovaries (HR 1.74, 95% CI 1.14-2.65).
Conclusion: Increased risk of earlier ovarian failure is a possible consequence of premenopausal hysterectomy. Although it is unresolved whether it is the surgery itself or the underlying condition leading to hysterectomy that is the cause of earlier ovarian failure, physicians and patients should take into account this possible sequela when considering options for treatment of benign conditions of the uterus.
Level of evidence: II.
Figures
References
-
- Whiteman MK, Hillis SD, Jamieson DJ, Morrow B, Podgornik MN, Brett KM, et al. Inpatient hysterectomy surveillance in the United States, 2000-2004. Am J Obstet Gynecol. 2008 Jan;198(1):34 e1–7. - PubMed
-
- Sample NI. Estimates for all discharges with any procedure code for abdominal and vaginal hysterectomy, Nationwide Inpatient Sample, 2009. 2009.
-
- Merrill RM, Layman AB, Oderda G, Asche C. Risk estimates of hysterectomy and selected conditions commonly treated with hysterectomy. Ann Epidemiol. 2008 Mar;18(3):253–60. - PubMed
-
- Keshavarz HHS, Burney A, Marchbanks P. Hysterectomy surveillance - United States, 1994-1999. Surveillance Summaries MMWR. 2002:1–7.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
