

The treatment of scaphoid nonunion using the Ilizarov fixator without bone graft, a study of 18 cases
- PMID: 22067958
- PMCID: PMC3224762
- DOI: 10.1186/1749-799X-6-57
The treatment of scaphoid nonunion using the Ilizarov fixator without bone graft, a study of 18 cases
Abstract
Objectives: Evaluating the safety and efficacy of the Ilizarov fine-wire compression/distraction technique in the treatment of scaphoid nonunion (SNU), without the use of bone graft.
Design: A retrospective review of 18 consecutive patients in one centre.
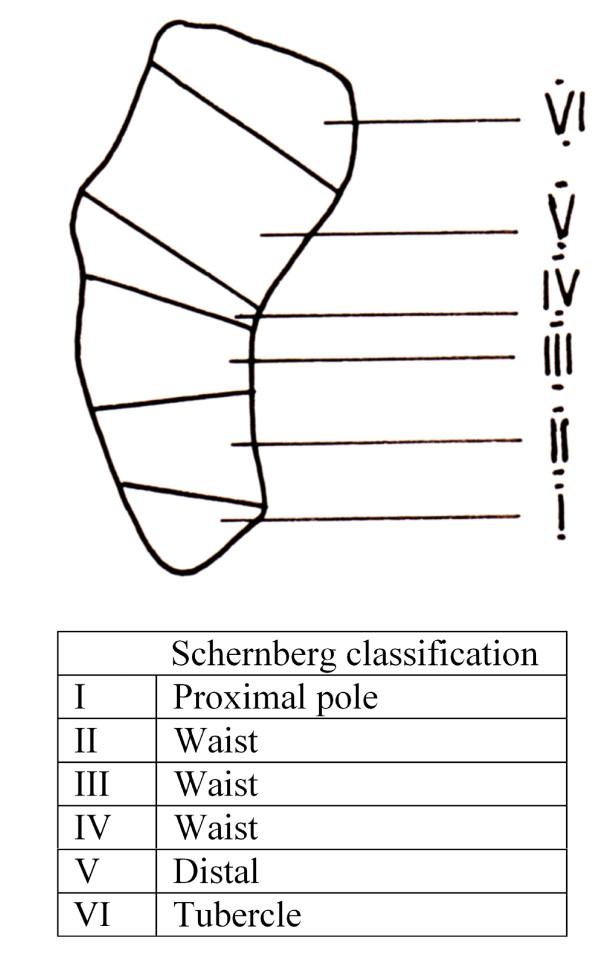
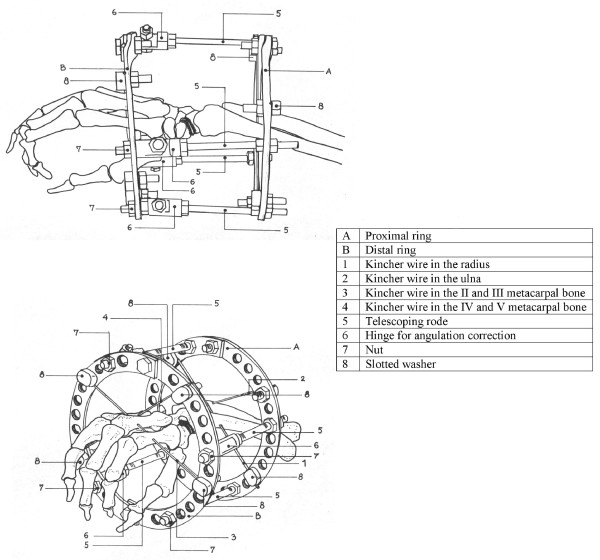
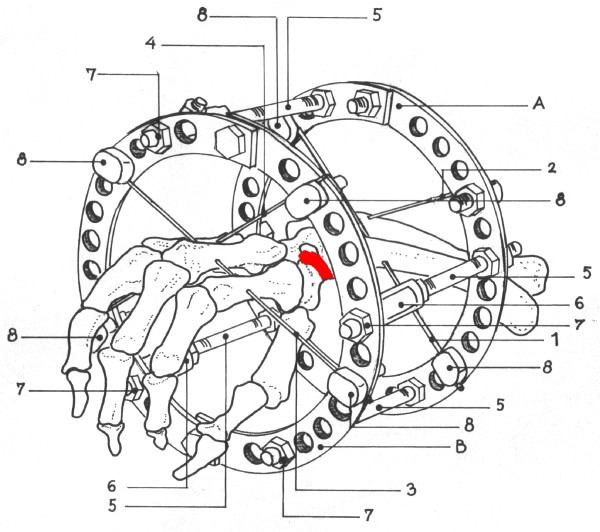
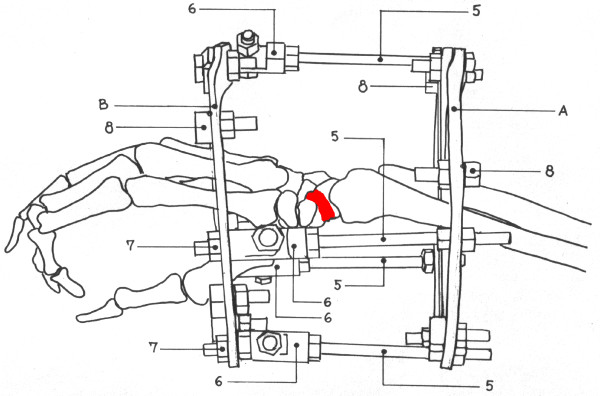
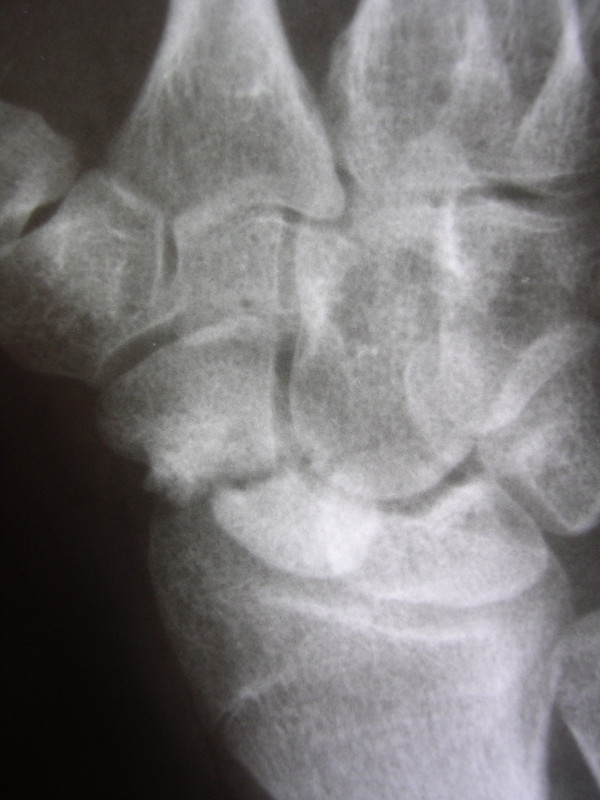
Patients and methods: 18 patients; 17 males; 1 female, with a mean SNU duration of 13.9 months. Patients with carpal instability, humpback deformity, carpal collapse, avascular necrosis or marked degenerative change, were excluded. Following frame application the treatment consisted of three stages: the frame was distracted 1 mm per day until radiographs showed a 2-3 mm opening at the SNU site (mean 10 days); the SNU site was then compressed for 5 days, at a rate of 1 mm per day, with the wrist in 15 degrees of flexion and 15 degrees of radial deviation; the third stage involved immobilization with the Ilizarov fixator for 6 weeks. The technique is detailed herein.
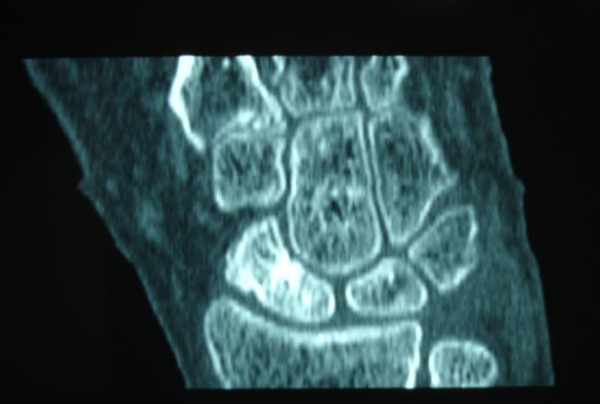
Results: Radiographic (CT) and clinical bony union was achieved in all 18 patients after a mean of 89 days (70-130 days). Mean modified Mayo wrist scores improved from 21 to 86 at a mean follow-up of 37 months (24-72 months), with good/excellent results in 14 patients. All patients returned to their pre-injury occupations and levels of activity at a mean of 117 days. Three patients suffered superficial K-wire infections, which resolved with oral antibiotics.
Conclusions: In these selected patients this technique safely achieved bony union without the need to open the SNU site and without the use of bone graft.
Figures

References
-
- Bond CD, Shin AY, McBride MT, Dao KD. Percutaneous screw fixation or cast immobilization for nondisplaced scaphoid fractures. J Bone Joint Surg Am. 2001;83-A(4):483–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
