Management of posterior fossa gliomas in children
- PMID: 22069433
- PMCID: PMC3208911
- DOI: 10.4103/1817-1745.85714
Management of posterior fossa gliomas in children
Abstract
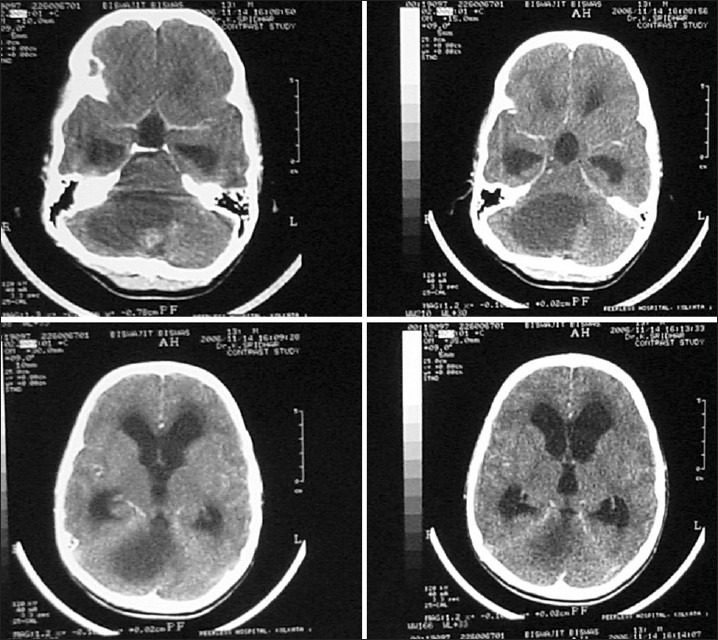
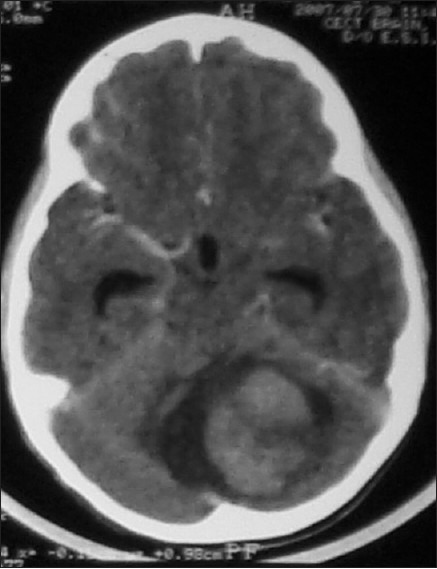
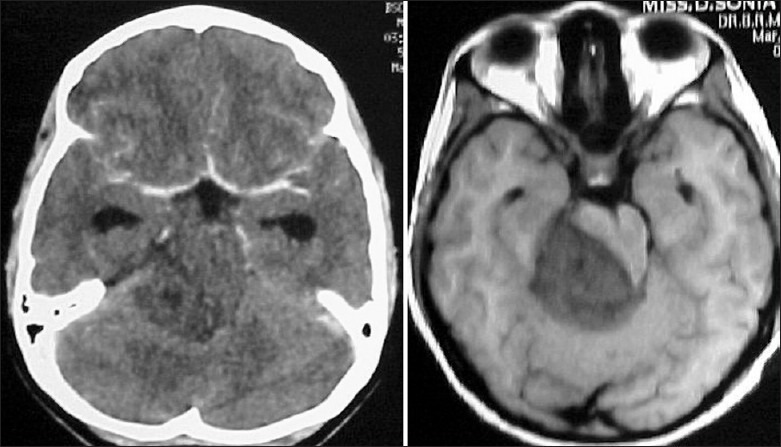
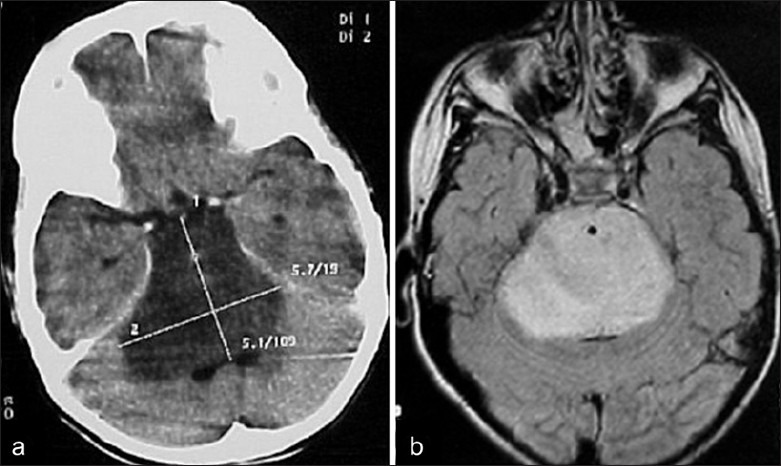
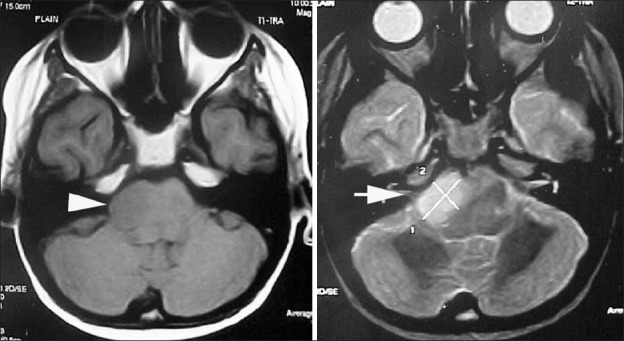
Brain tumours form the most common type of solid tumour in children and more that 50% of these are infratentorial. Cerebellar astrocytomas and brain stem gliomas are the commonest posterior fossa glial tumours in children. Cerebellar astrocytomas represent up to 10% of all primary brain tumours and up to 25% of posterior fossa tumors in children, with Low grade gliomas forming the commonest of the cerebellar gliomas. They commonly present with symptoms and signs of raised intracranial pressure due to obstructive hydrocephalus. Radiologically they may be solid or cystic with or without a mural nodule. Surgical excision is the mainstay of treatment and forms the most consistent factor influencing progression free and long term survival. While majority of the tumours are pilocytic astrocytomas, they may also be fibrillary astrocytomas or even high grade tumours. Tumour histology does not appear to be an independent factor in the prognosis of these children, and therefore no palliative treatment after surgery is advocated. Brain stem gliomas account for approximately 10% of all pediatric brain tumours. Cranial nerve signs, ataxia and cerebellar signs with or without symptoms and signs of raised intracranial pressure are classically described symptoms and signs. Radiographic findings and clinical correlates can be used to categorize brain stem tumours into four types: diffuse, focal, exophytic and cervicomedullary. Histologically most brain stem gliomas are fibrillary astrocytomas. Diffuse brain stem gliomas are the most commonly seen tumour in the brain stem. These lesions are malignant high grade fibrillary astrocytomas. Focal tumours of the brain stem are demarcated lesions generally less than 2 cms in size, without associated edema. Most commonly seen in the midbrain or medulla, they form a heterogeneous pathological group, showing indolent growth except when the lesion is a PNET. Dorsally exophytic tumours lie in the fourth ventricle, while cervicomedullary lesions are similar to spinal intramedullary tumours. Expanding lesions are the only lesions amenable for excision while infiltrative and ventral lesions are not.
Keywords: Brain Stem gliomas; Cerebellar gliomas; Pediatric; Pilocytic astrocytoma; Pontine gliomas.
Conflict of interest statement
Figures


References
-
- Pollack IF. The role of surgery in pediatric gliomas. J Neurooncol. 1999;42:271–88. - PubMed
-
- Pollack IF. Brain tumours in children. N Engl J Med. 1994;331:1500–7. - PubMed
-
- Duffner PK, Cohen ME, Myers MH, Heise HW. Survival of children with brain tumors: SEER program. 1973-1980. Neurology. 1986;36:597–601. - PubMed