

Continuous nasogastric milk feeding versus intermittent bolus milk feeding for premature infants less than 1500 grams
- PMID: 22071802
- PMCID: PMC7066504
- DOI: 10.1002/14651858.CD001819.pub2
Continuous nasogastric milk feeding versus intermittent bolus milk feeding for premature infants less than 1500 grams
Update in
-
Continuous nasogastric milk feeding versus intermittent bolus milk feeding for preterm infants less than 1500 grams.Cochrane Database Syst Rev. 2021 Jun 24;6(6):CD001819. doi: 10.1002/14651858.CD001819.pub3. Cochrane Database Syst Rev. 2021. PMID: 34165778 Free PMC article.
Abstract
Background: Milk feedings can be given via nasogastric tube either intermittently, typically over 10 to 20 minutes every two or three hours, or continuously, using an infusion pump. Although theoretical benefits and risks of each method have been proposed, effects on clinically important outcomes remain uncertain.
Objectives: To examine the evidence regarding the effectiveness of continuous versus intermittent bolus nasogastric milk feeding in premature infants less than 1500 grams.
Search methods: Searches were performed of the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, Issue 3, 2011), MEDLINE, CINAHL and HealthSTAR up to July 2011.
Selection criteria: Randomised and quasi-randomised clinical trials comparing continuous versus intermittent bolus nasogastric milk feeding in premature infants less than 1500 grams.
Data collection and analysis: Two review authors independently assessed all trials for relevance and methodologic quality. The standard methods of the Cochrane Neonatal Review Group were used to extract data.
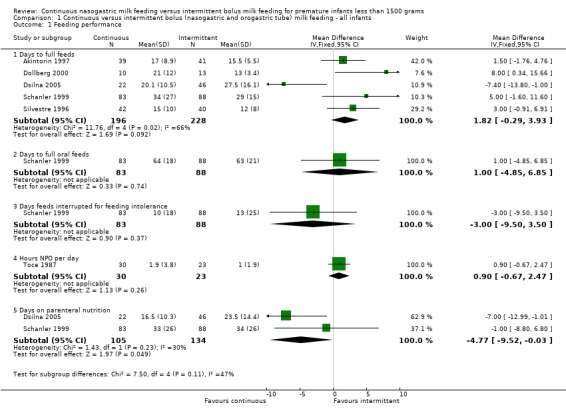
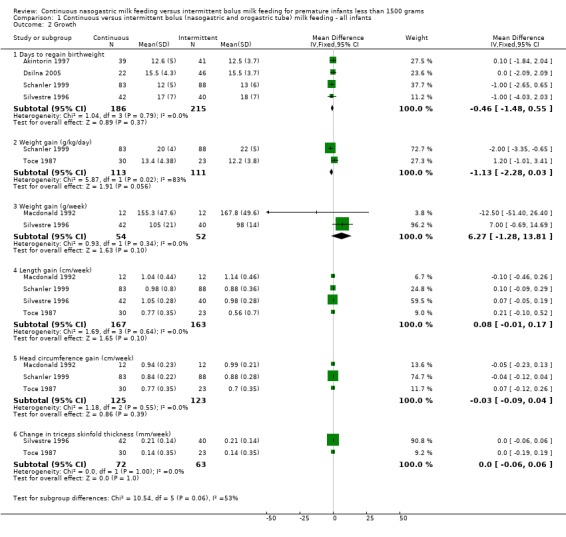
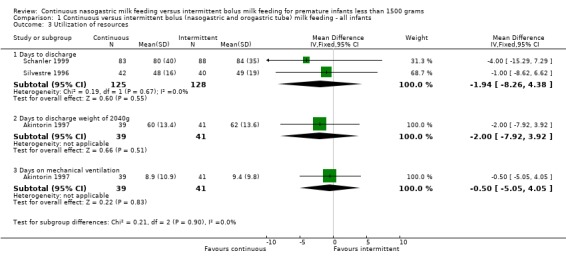
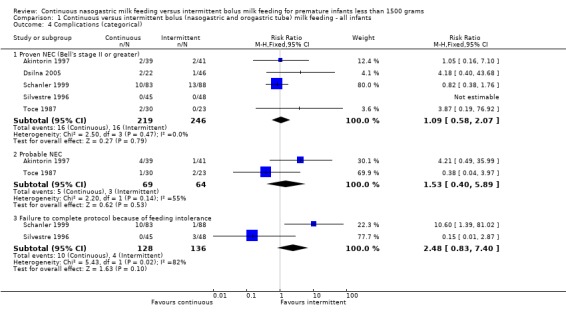
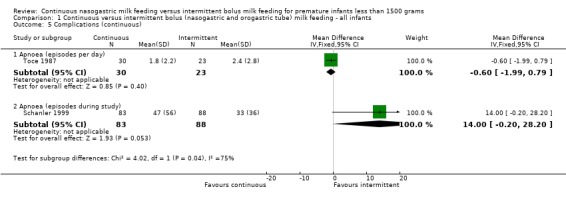
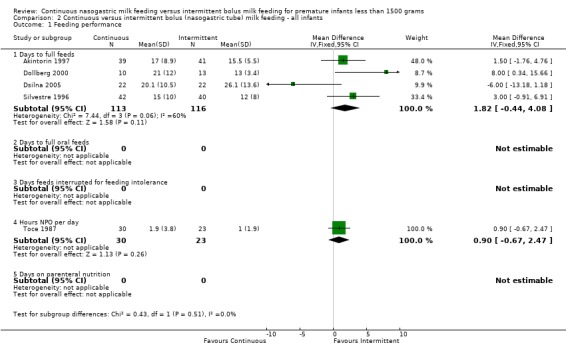
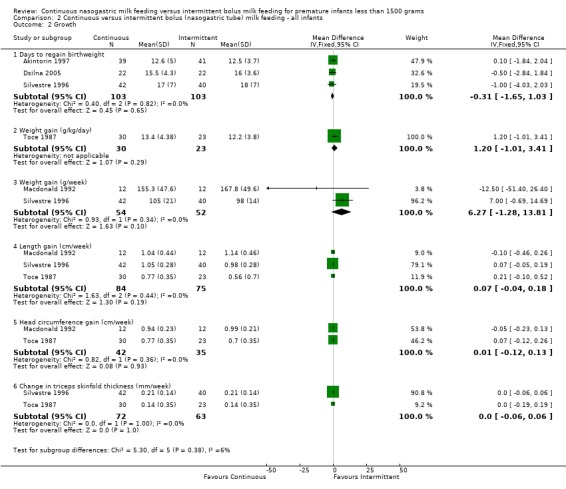
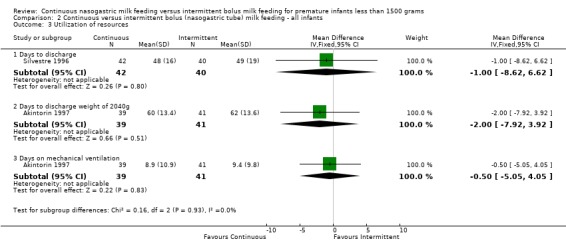
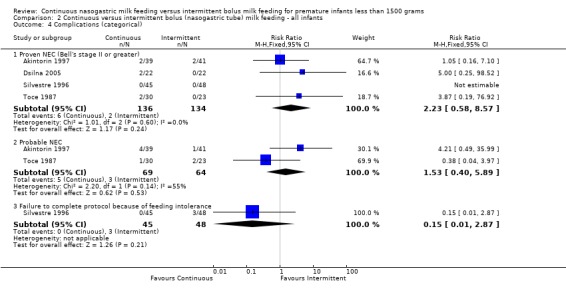
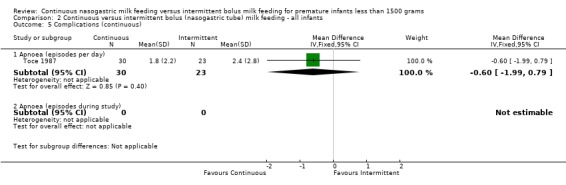
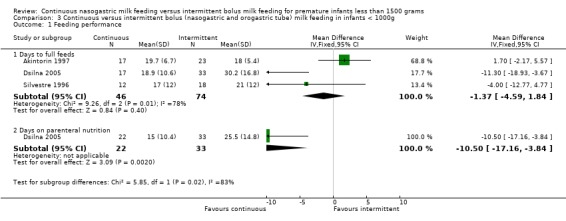
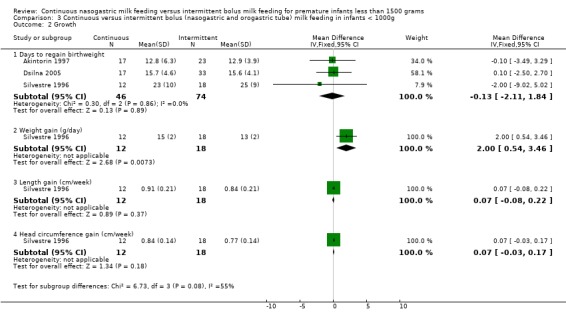
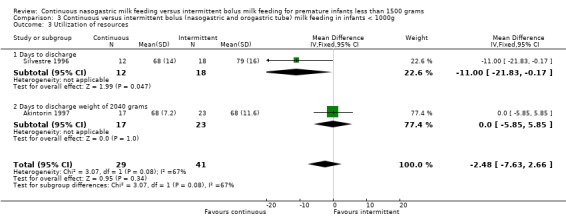
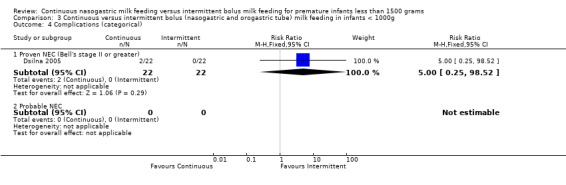
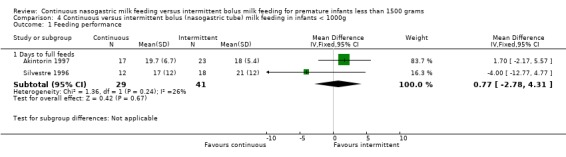
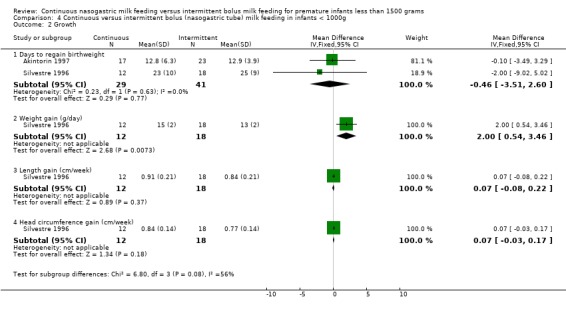
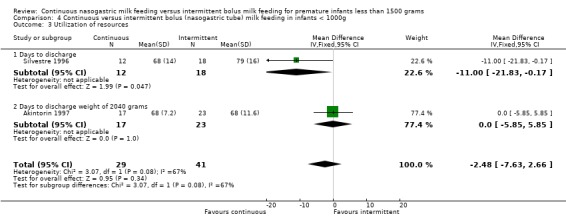
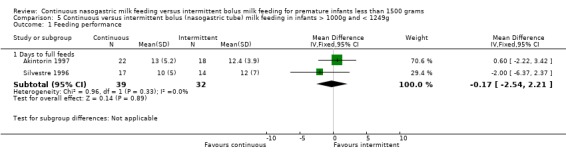
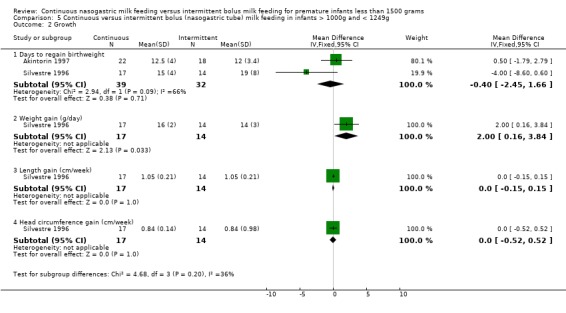
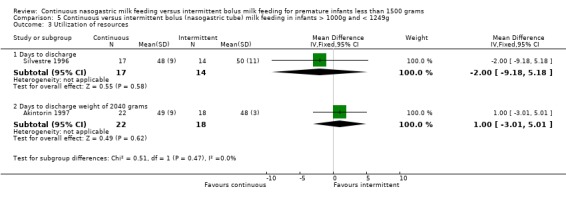
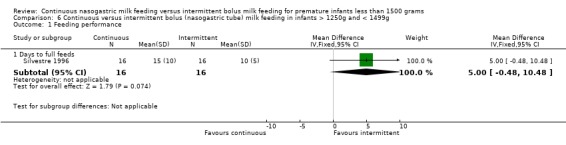
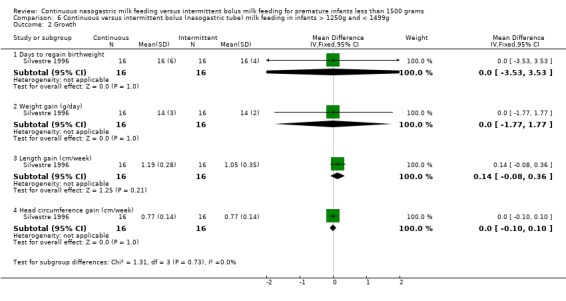
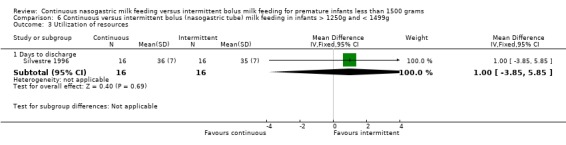
Main results: Overall, the seven included trials, involving 511 infants, found no differences in time to achieve full enteral feeds between feeding methods (weighted mean difference (WMD) 2 days; 95% CI -0.3 to 3.9) . In the subgroup analysis of those studies comparing continuous nasogastric versus intermittent bolus nasogastric milk feedings the findings remained unchanged (WMD 2 days, 95% CI -0.4 to 4.1). There was no significant difference in somatic growth and incidence of NEC between feeding methods irrespective of tube placement. One study noted a trend toward more apneas during the study period in infants fed by the continuous tube feeding method compared to those fed by intermittent feedings delivered predominantly by orogastric tube placements [mean difference (MD) 14.0 apneas during study period; 95% CI -0.2 to 28.2]. In subgroup analysis based on weight groups, one study suggested that infants less than 1000 grams and 1000 to 1250 grams birth weight gained weight faster when fed by the continuous nasogastric tube feeding method compared to intermittent nasogastric tube feeding method (MD 2.0 g/day; 95% CI 0.5 to 3.5; MD 2.0 g/day; 95% CI 0.2 to 3.8, respectively). A trend toward earlier discharge for infants less than 1000 grams birth weight fed by the continuous tube feeding method compared to intermittent nasogastric tube feeding method (MD -11 days; 95% CI -21.8 to -0.2).
Authors' conclusions: Small sample sizes, methodologic limitations, inconsistencies in controlling variables that may affect outcomes, and conflicting results of the studies to date make it difficult to make universal recommendations regarding the best tube feeding method for premature infants less than 1500 grams. The clinical benefits and risks of continuous versus intermittent nasogastric tube milk feeding cannot be reliably discerned from the limited information available from randomised trials to date.
Conflict of interest statement
None
Figures
Update of
-
Continuous nasogastric milk feeding versus intermittent bolus milk feeding for premature infants less than 1500 grams.Cochrane Database Syst Rev. 2003;(1):CD001819. doi: 10.1002/14651858.CD001819. Cochrane Database Syst Rev. 2003. Update in: Cochrane Database Syst Rev. 2011 Nov 09;(11):CD001819. doi: 10.1002/14651858.CD001819.pub2. PMID: 12535414 Updated.
References
References to studies included in this review
Akintorin 1997 {published data only}
-
- Akintorin SM, Kamat M, Pildes RS, Kling P, Andes S, Hill J, Pyati S. A prospective randomized trial of feeding methods in very low birth weight infants. Pediatrics 1997;100:E4. - PubMed
Dollberg 2000 {published and unpublished data}
-
- Dollberg S, Kuint J, Mazkereth R, et al. Feeding tolerance in preterm infants: Randomized trial of bolus and continuous feeding. Journal of the American College of Nutrition 2000;19(6):797‐800. - PubMed
Dsilna 2005 {published and unpublished data}
-
- Dsilna A, Christensson K, Alfredsson L, et al. Continuous feeding promotes gastrointestinal tolerance and growth in very low birth weight infants. Journal of Pediatrics 2005;147:43‐9. - PubMed
Macdonald 1992 {published and unpublished data}
Schanler 1999 {published and unpublished data}
-
- Schanler RJ, Shulman RJ, Lau C. Feeding strategies for premature infants: Beneficial outcomes of feeding fortified milk versus preterm formula. Pediatrics 1999;103:1150‐7. - PubMed
-
- Schanler RJ, Shulman RJ, Lau C, Smith EO, Heitkemper MM. Feeding strategies for premature infants: Randomized trial of gastrointestinal priming and tube‐feeding method. Pediatrics 1999;103(2):434‐9. - PubMed
-
- Shulman RJ, Schanler RJ, Lau C, Heitkemper M, Ou CN, Smith EO. Early feeding, antenatal glucocorticoids, and human milk decrease intestinal permeability in preterm infants. Pediatric Research 1998;44:519‐23. - PubMed
Silvestre 1996 {published data only}
-
- Silvestre MA, Morbach CA, Brans YW, Shankaran S. A prospective randomized trial comparing continuous versus intermittent feeding method in very low birth weight neonates. Journal of Pediatrics 1996;128:748‐52. - PubMed
Toce 1987 {published data only}
-
- Toce SS, Keenan WJ, Homan SM. Enteral feeding in very‐low‐birth‐weight infants. A comparison of two nasogastric methods. American Journal of Diseases of Children 1987;141:439‐44. - PubMed
References to studies excluded from this review
Baker 1997 {published data only}
-
- Baker JH, Berseth CL. Duodenal motor responses in preterm infants fed formula with varying concentrations and rates of infusion. Pediatric Research 1997;42:618‐22. - PubMed
Berseth 1992 {published data only}
-
- Berseth CL, Baker J, DeVille K, et al. Rate of feeding and nutrient concentration affect preterm small intestinal motor responses to orogastric feedings. Gastroenterology 1992;103:1385(Abstract).
Dsilna 2008 {published data only}
-
- Dsilna A, Christensson K, Gustafsson AS, Lagercrantz H, Alfredsson L. Behavioural stress is affected by the mode of tube feeding in very low birth weight infants. Clinical Journal of Pain 2008;24:447‐55. - PubMed
Additional references
Aynsley‐Green 1982
-
- Aynsley‐Green A, Adrian TE, Bloom SR. Feeding and the development of enteroinsular hormone secretion in the preterm infant: Effects of continuous gastric infusions of human milk compared with intermittent boluses. Acta Paediatrica Scandinavica 1982;71:379‐83. - PubMed
Aynsley‐Green 1989
-
- Aynsley‐Green A. New insights into the nutritional management of newborn infants derived from studies of metabolic and endocrine inter‐relations during the adaptation of postnatal life. The Proceedings of the Nutrition Society 1989;48:283‐92. - PubMed
Aynsley‐Green 1990
-
- Aynsley‐Green A, Lucas A, Lawson GR, Bloom SR. Gut hormones and regulatory peptides in relation to enteral feeding, gastroenteritis, and necrotizing enterocolitis in infancy. Journal of Pediatrics 1990;117:S24‐32. - PubMed
Grant 1991
-
- Grant J, Denne SC. Effect of intermittent versus continuous enteral feeding on energy expenditure in premature infants. Journal of Pediatrics 1991;118:928‐32. - PubMed
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org, [updated March 2011].
Krishnan 1981
-
- Krishnan V, Satish M. Continuous (C) vs. intermittent (I) nasogastric (N/G) feeding in very low birth weight (VLBW) infants. Pediatric Research 1981;15:537 (Abstract).
Lucas 1986
-
- Lucas A, Bloom SR, Aynsley‐Green A. Gut hormones and "minimal enteral feeding". Acta Paediatrica Scandinavica 1986;75:719‐23. - PubMed
Newell 1988
Raudonis 1995
-
- Raudonis BM, Talbot LA. Use of critical thinking in research: The research critique. In: Talbot LA editor(s). Principles and practice of nursing research. St. Louis: Mosby, 1995:513‐534.
Urrutia 1983
-
- Urrutia J, Poole E. Continuous nasogastric versus intermittent gavage feedings in very low birth weight infants. Pediatric Research 1983;17:203A (Abstract).
References to other published versions of this review
Premji 2001
Premji 2003
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical