

Triphasic versus monophasic oral contraceptives for contraception
- PMID: 22071807
- PMCID: PMC7154342
- DOI: 10.1002/14651858.CD003553.pub3
Triphasic versus monophasic oral contraceptives for contraception
Abstract
Background: Side effects of oral contraceptive (OC) pills discourage adherence to and continuation of OC regimens. Strategies to decrease adverse effects led to the introduction of the triphasic OC in the 1980s. Whether triphasic OCs have higher accidental pregnancy rates than monophasic pills is unknown. Nor is it known if triphasic pills give better cycle control and fewer side effects than the monophasic pills.
Objectives: To compare triphasic OCs with monophasic OCs in terms of efficacy, cycle control, and discontinuation due to side effects.
Search methods: We searched the computerized databases of the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library), MEDLINE, POPLINE, EMBASE, and LILACS, as well as clinical trials databases (ClinicalTrials.gov and the World Health Organization Clinical Trials Registry Platform (ICTRP)) in May 2011. Additionally, we searched the reference lists of relevant articles. We also contacted researchers and pharmaceutical companies to identify other trials not found in our search.
Selection criteria: We included randomized controlled trials (RCTs) comparing any triphasic OC with any monophasic pill used to prevent pregnancy. Interventions had to include at least three treatment cycles.
Data collection and analysis: We assessed the studies found in the literature searches for possible inclusion and for their methodological quality. We contacted the authors of all included studies and of possibly randomized trials for supplemental information about the methods used and outcomes studied. We entered the data into RevMan and calculated odds ratios for the outcome measures of efficacy, breakthrough bleeding, spotting, withdrawal bleeding and discontinuation.
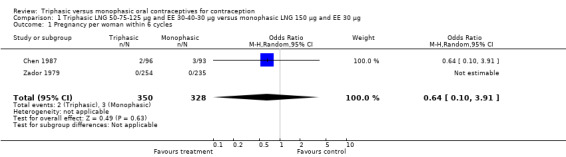
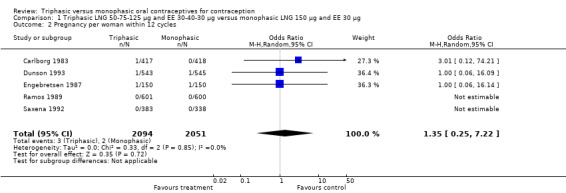
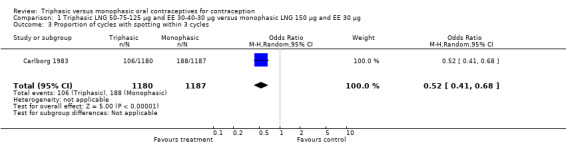
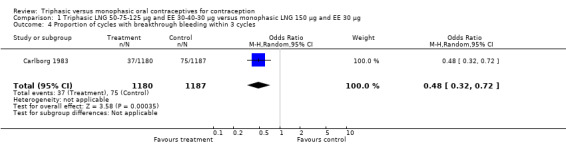
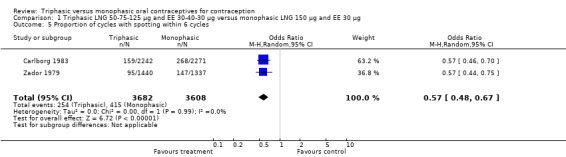
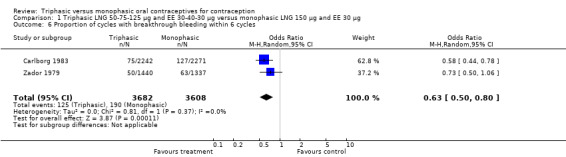
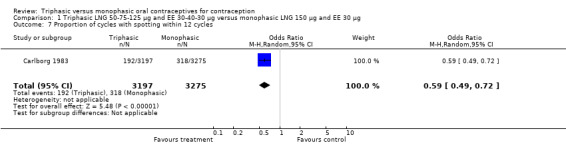
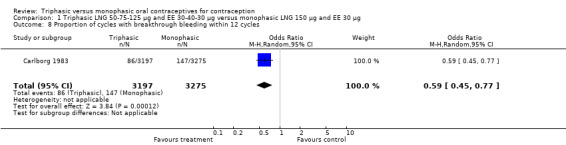
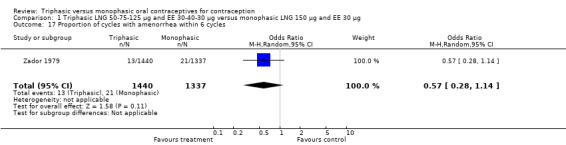
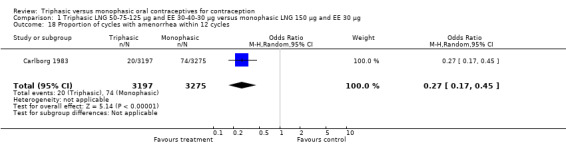
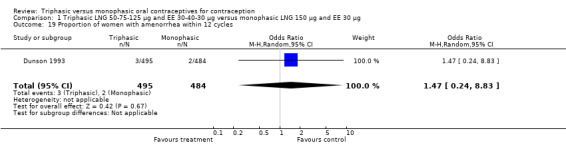
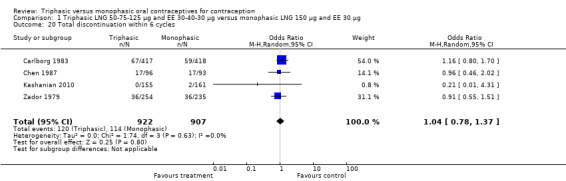
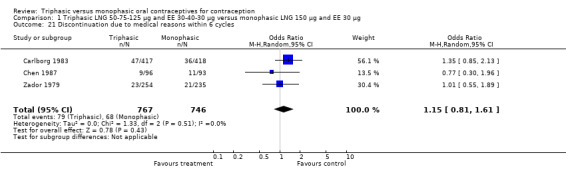
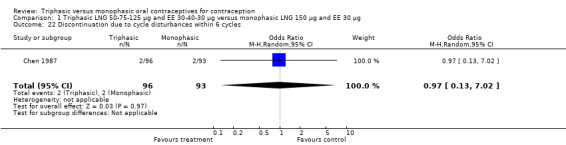
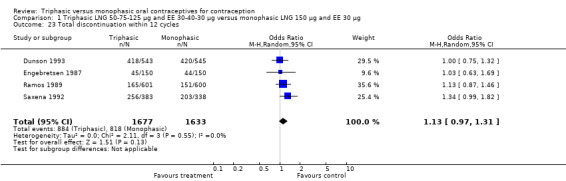
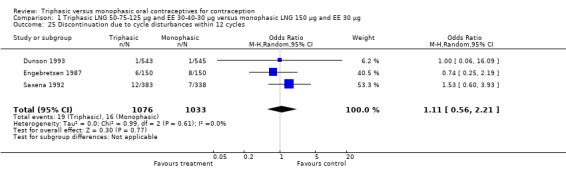
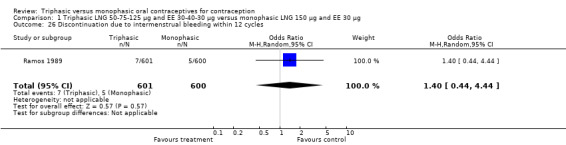
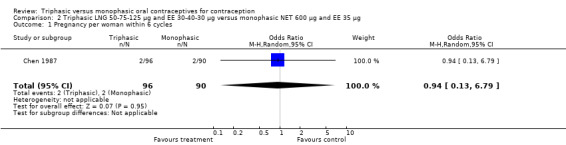
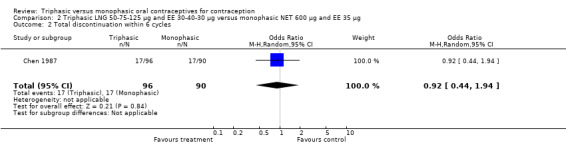
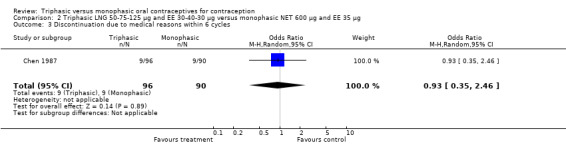
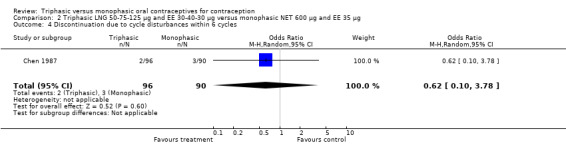
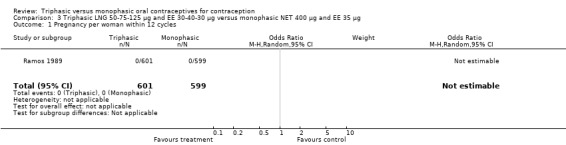
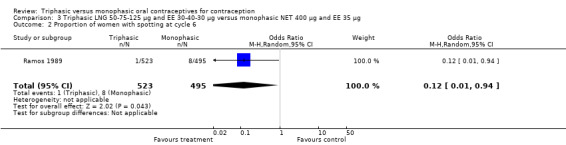
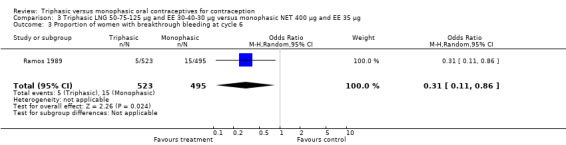
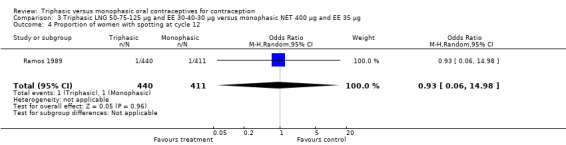
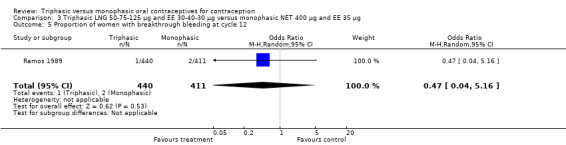
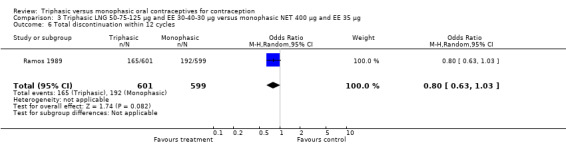
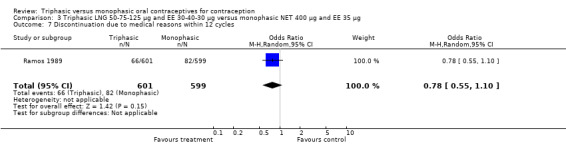
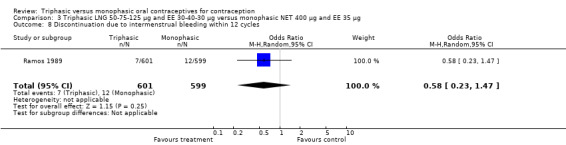
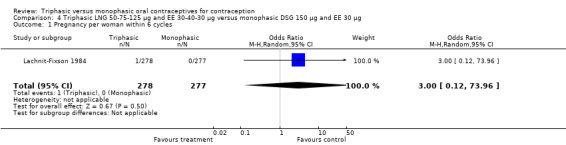
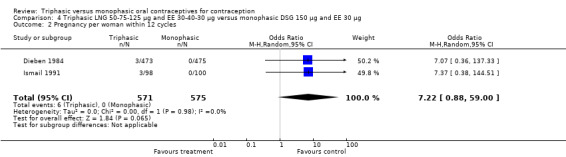
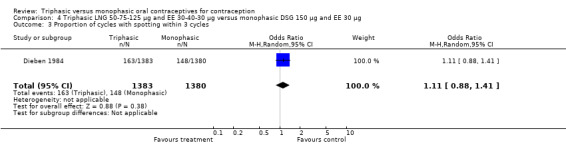
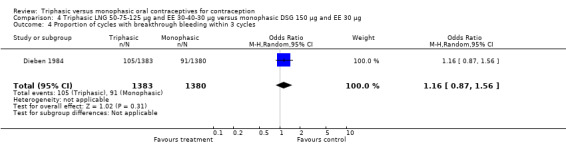
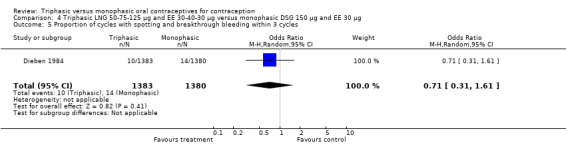
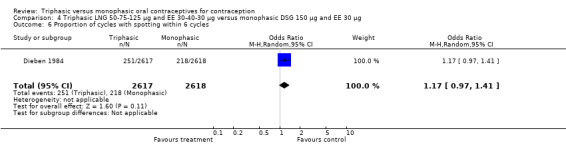
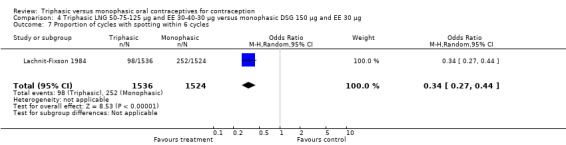
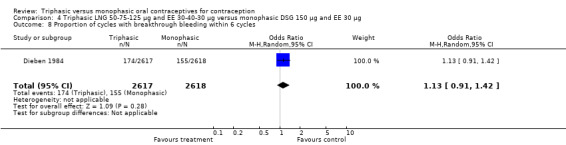
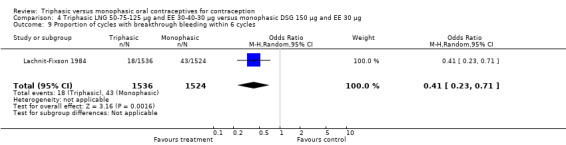
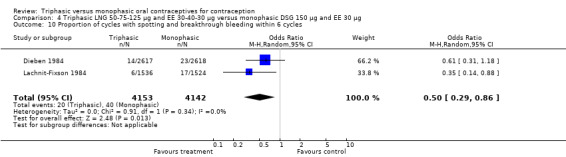
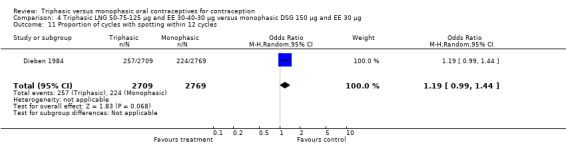
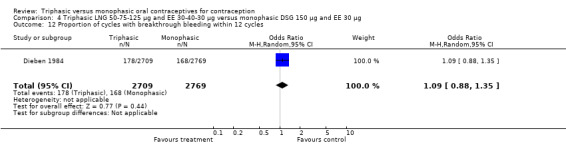
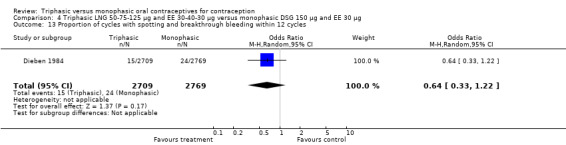
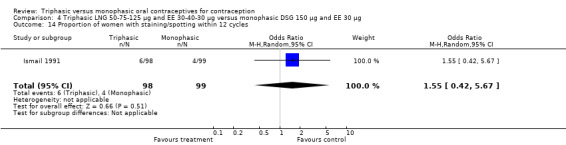
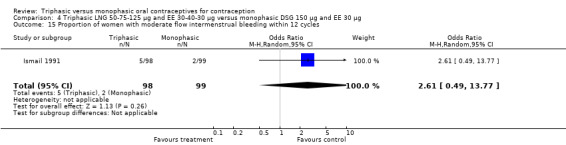
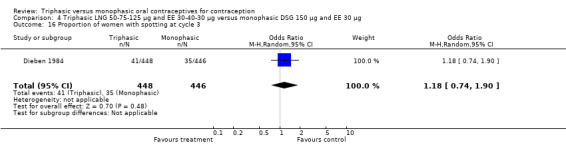
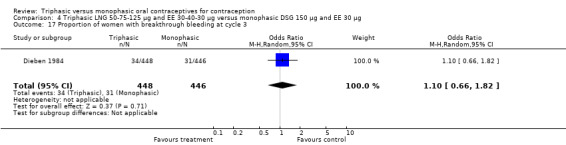
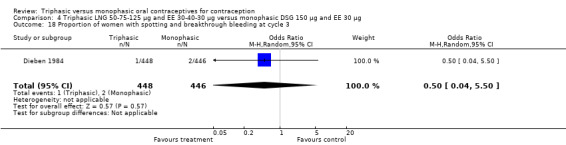
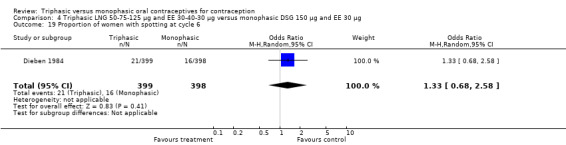
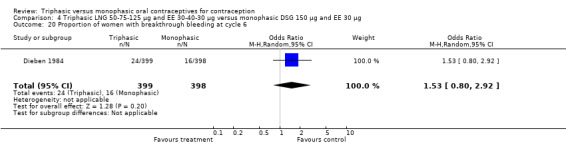
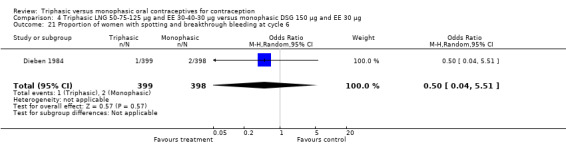
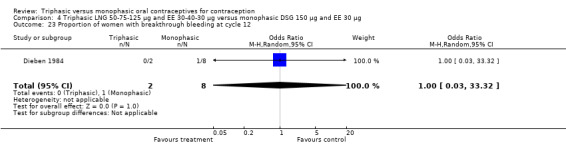
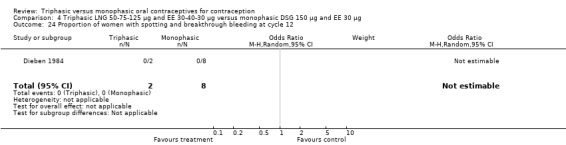
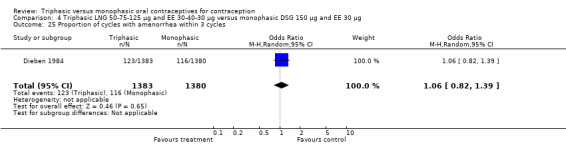
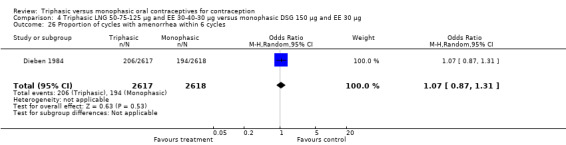
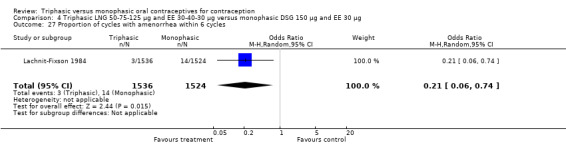
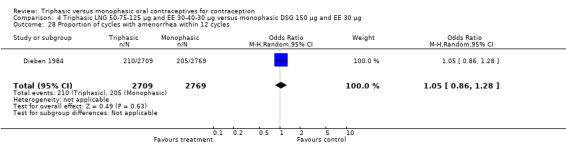
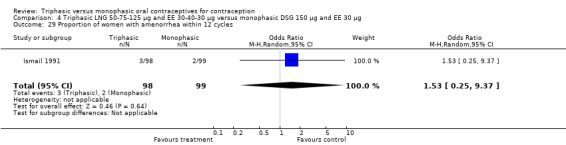
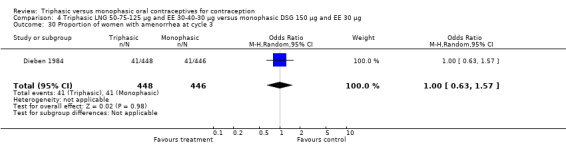
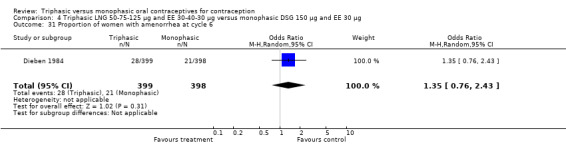
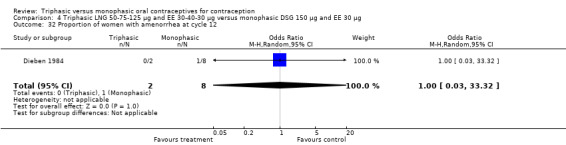
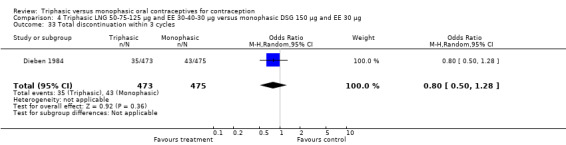
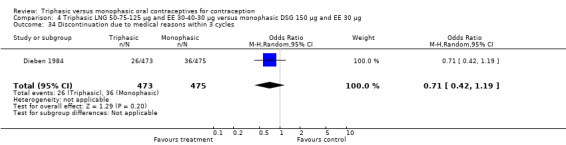
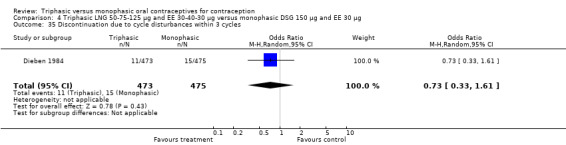
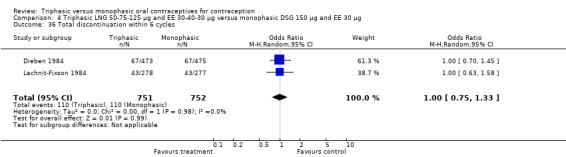
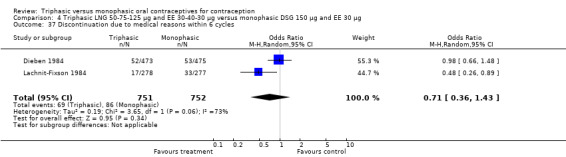
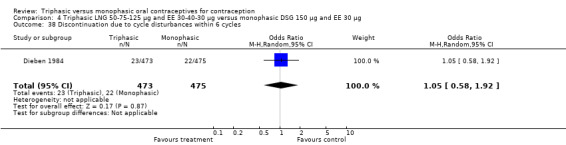
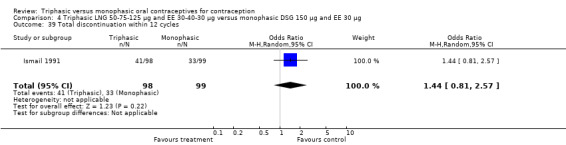
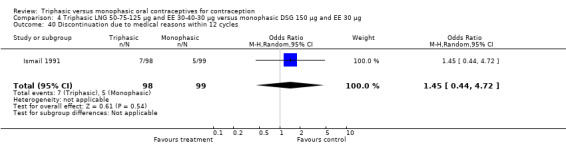
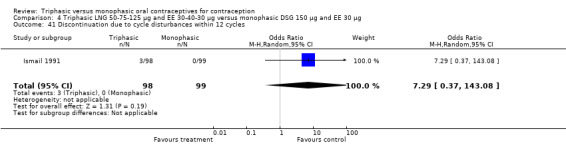
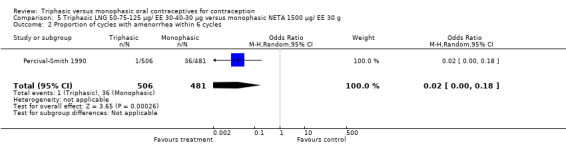
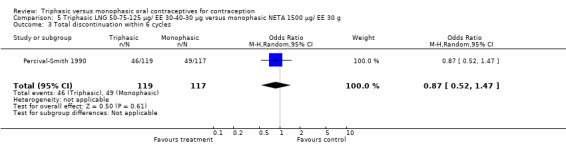
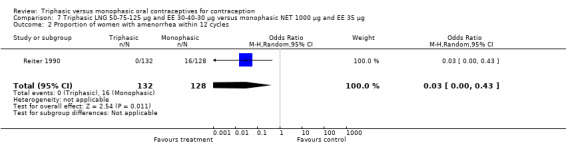
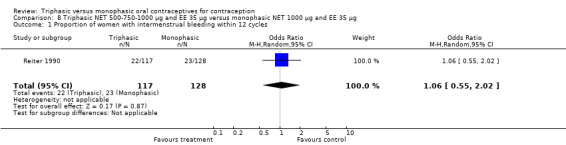
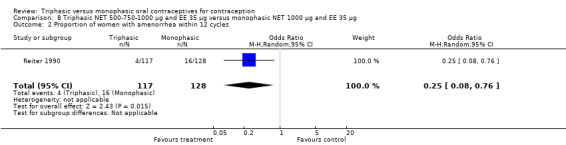
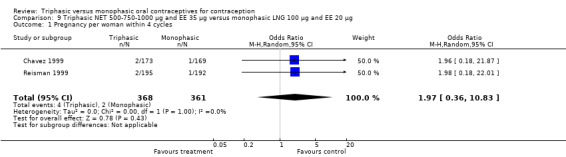
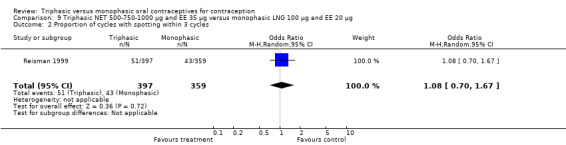
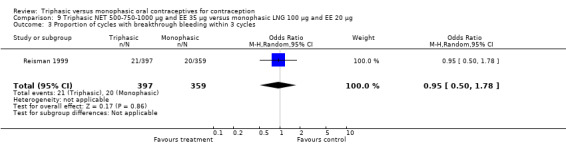
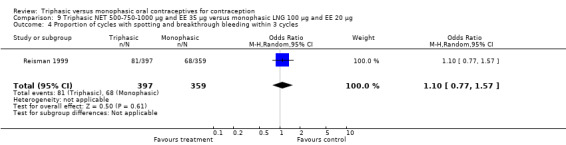
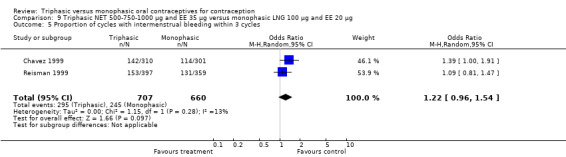
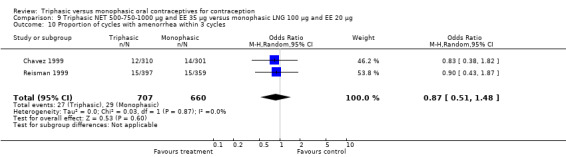
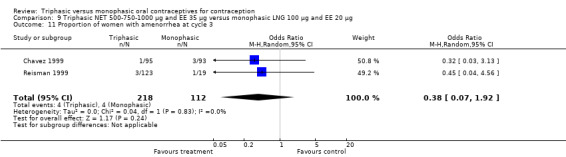
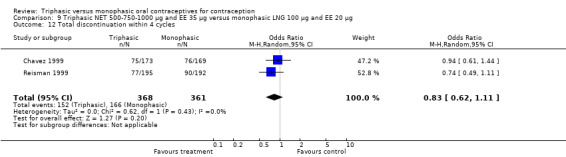
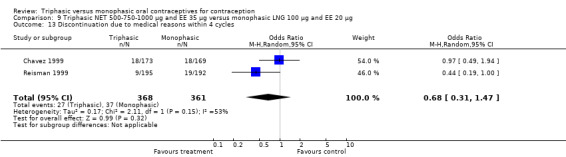
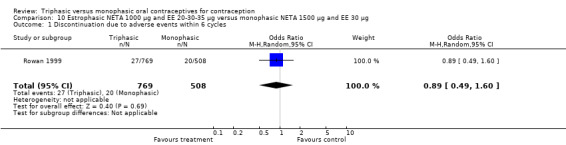
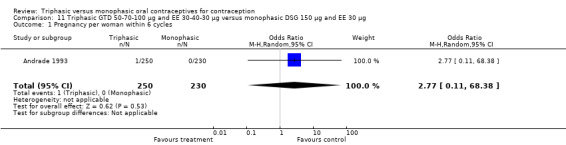
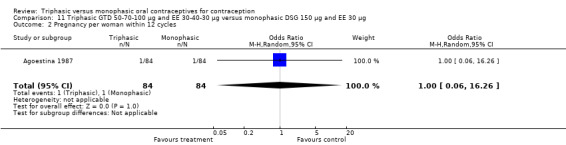
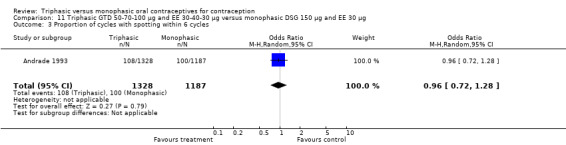
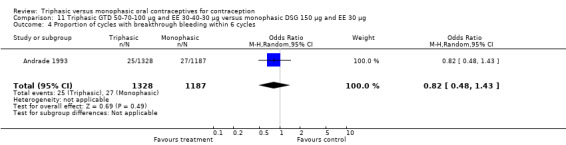
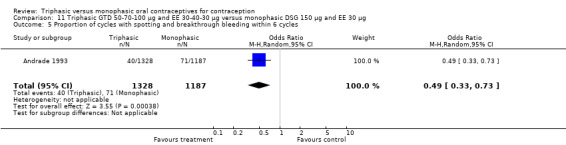
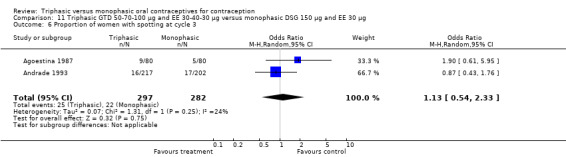
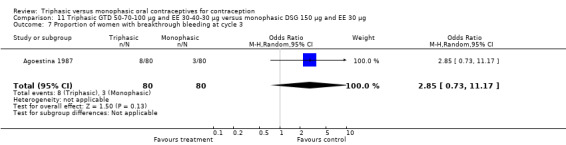
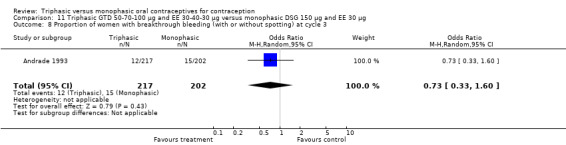
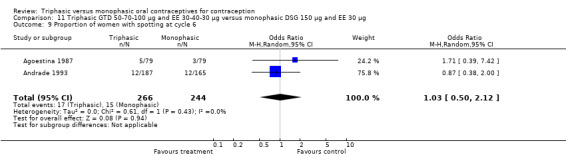
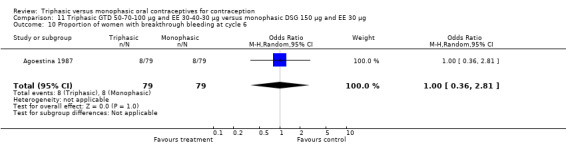
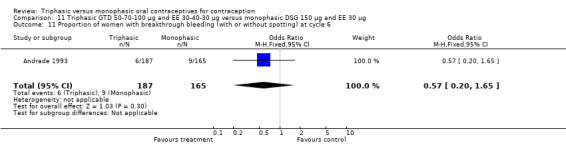
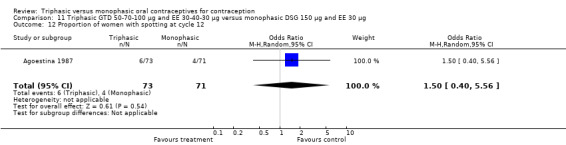
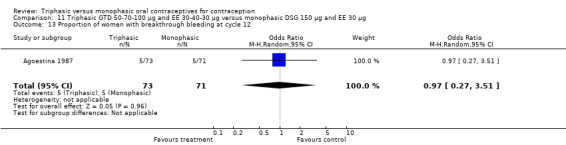
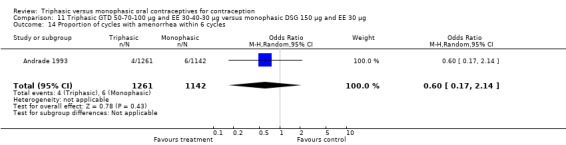
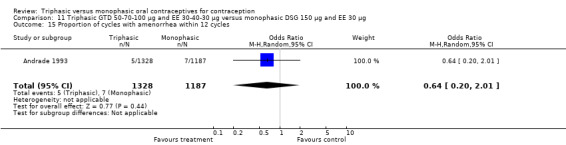
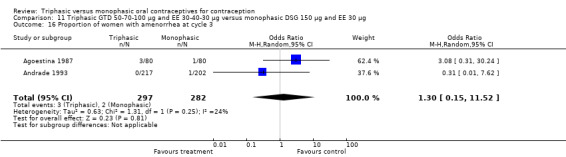
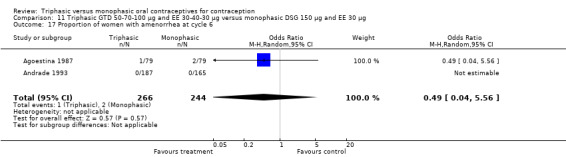
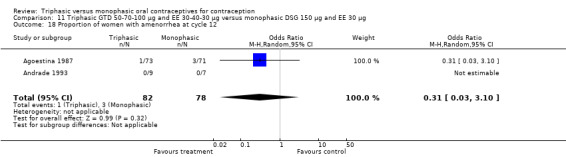
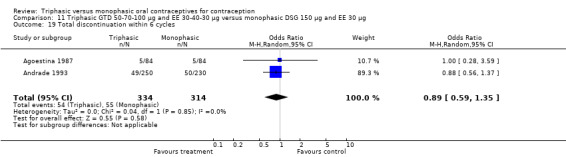
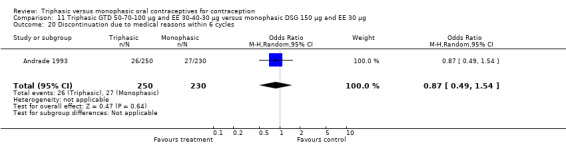
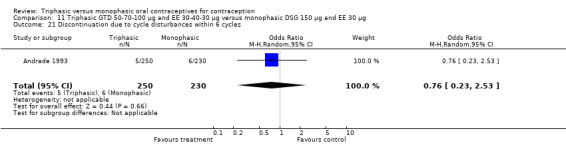
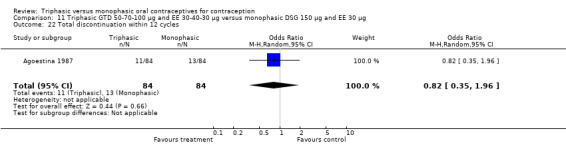
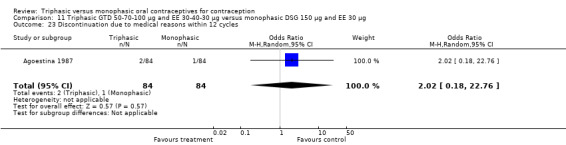
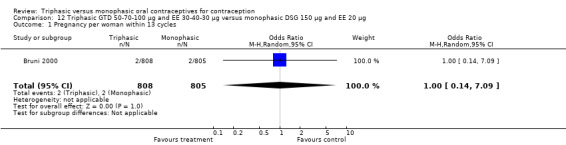
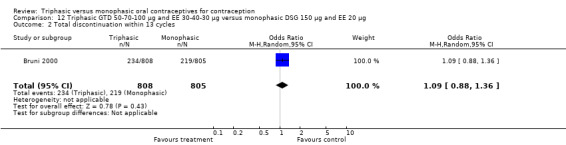
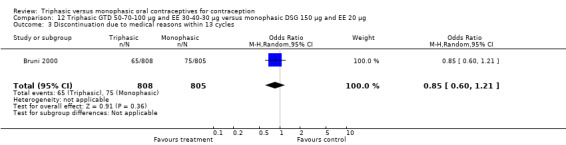
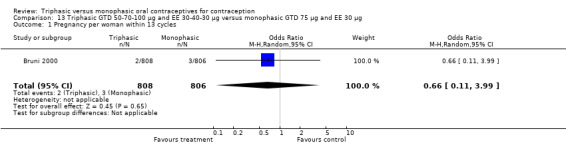
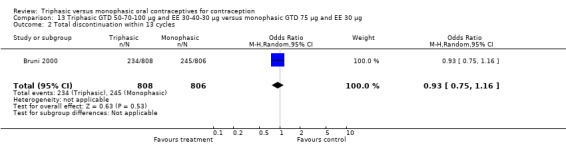
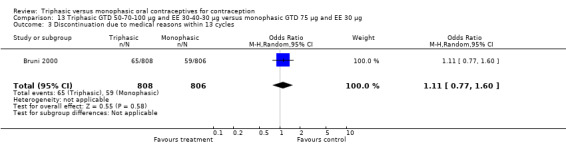
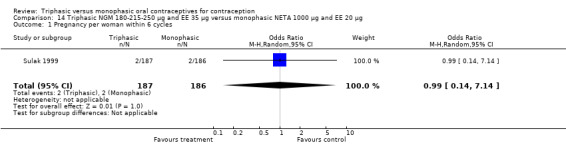
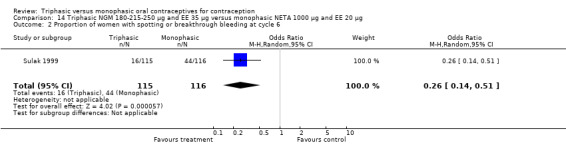
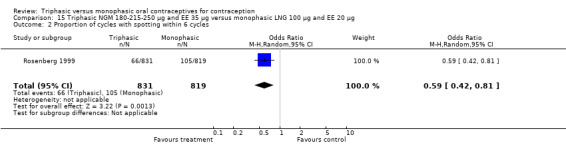
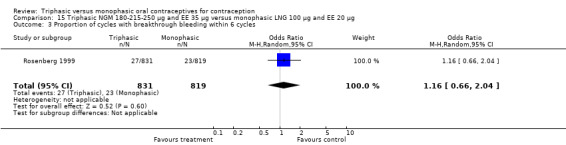
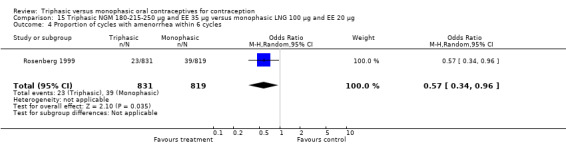
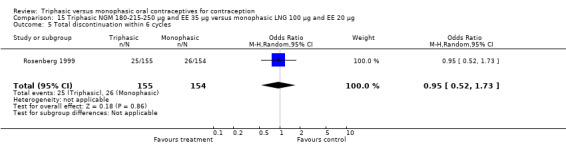
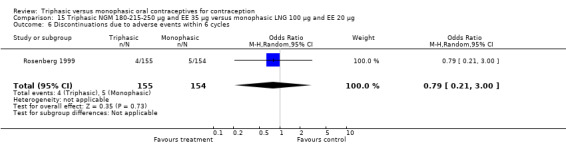
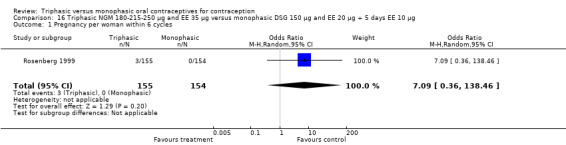
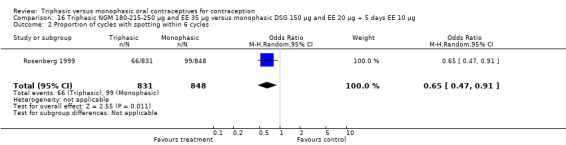
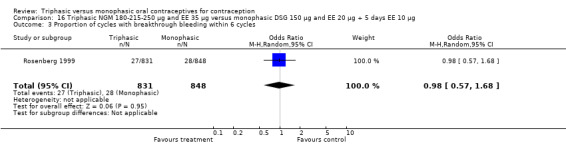
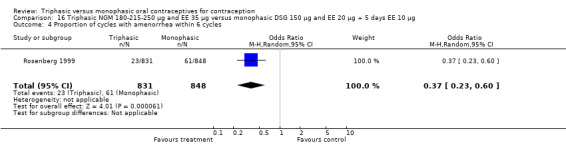
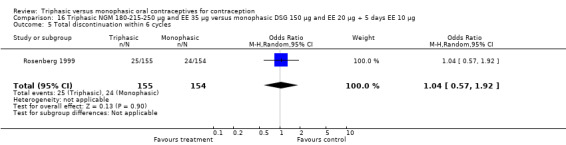
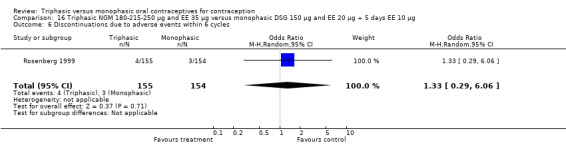
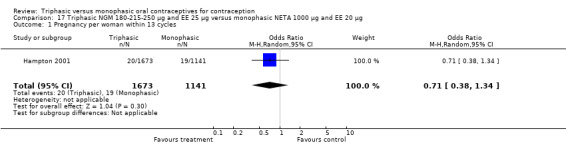
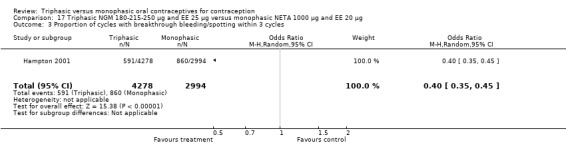
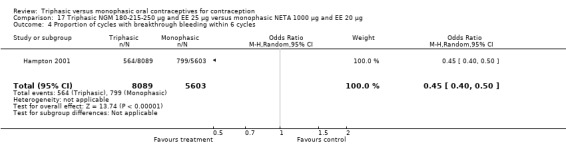
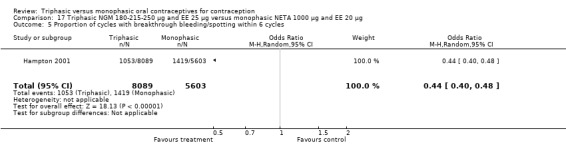
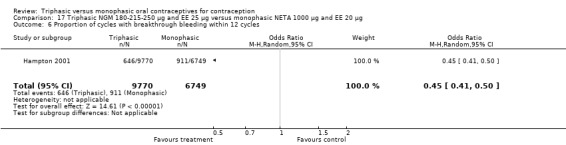
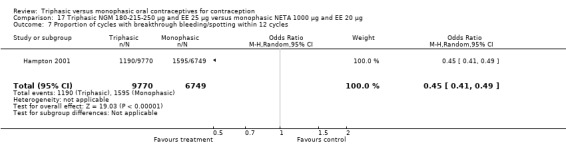
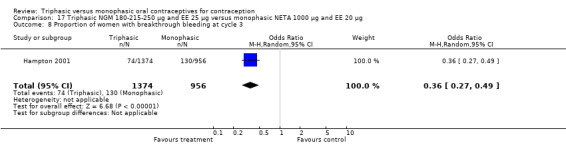
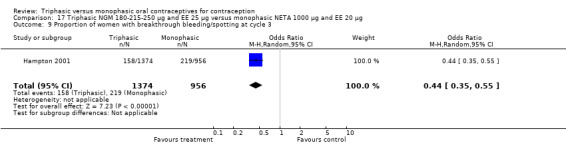
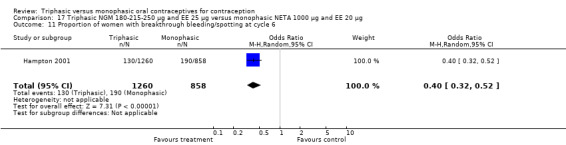
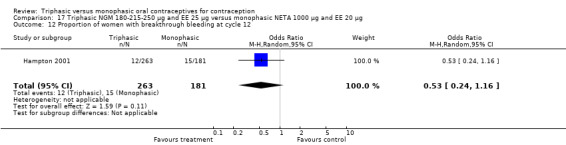
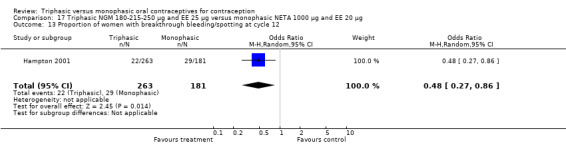
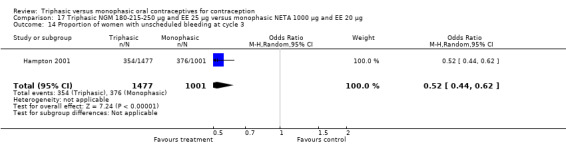
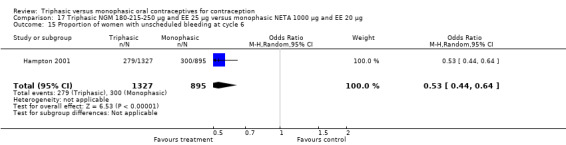
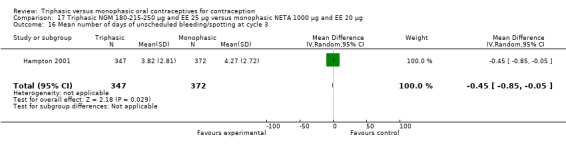
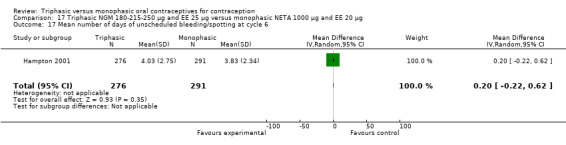
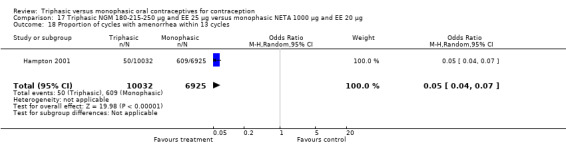
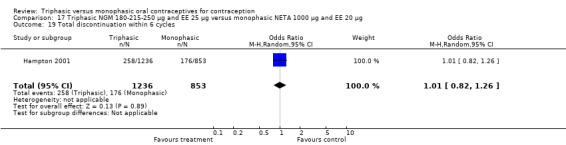
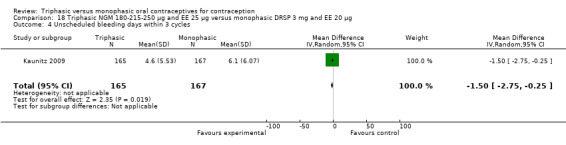
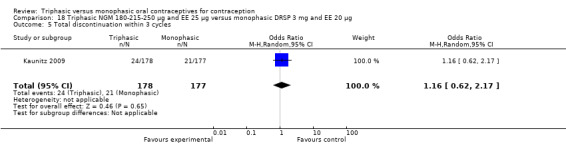
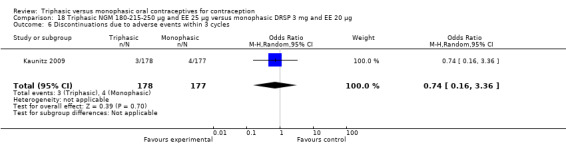
Main results: Of 23 trials included, 19 examined contraceptive effectiveness. The triphasic and monophasic preparations did not differ significantly. Several trials reported favorable bleeding patterns, that is less spotting, breakthrough bleeding or amenorrhea, in triphasic versus monophasic OC users. However, meta-analysis was generally not possible due to differences in measuring and reporting the cycle disturbance data as well as differences in progestogen type and hormone dosages. No significant differences were found in the numbers of women who discontinued due to medical reasons, cycle disturbances, intermenstrual bleeding or adverse events.
Authors' conclusions: The available evidence is insufficient to determine whether triphasic OCs differ from monophasic OCs in effectiveness, bleeding patterns or discontinuation rates. Therefore, we recommend monophasic pills as a first choice for women starting OC use. Large, high-quality RCTs that compare triphasic and monophasic OCs with identical progestogens are needed to determine whether triphasic pills differ from monophasic OCs. Future studies should follow the recommendations of Belsey or Mishell on recording menstrual bleeding patterns and the CONSORT reporting guidelines.
Conflict of interest statement
DA Grimes has consulted with the pharmaceutical companies Bayer Healthcare Pharmaceuticals and Merck & Co, Inc.
Three of the authors (DA Grimes, KF Schulz, LM Lopez) are employed by FHI 360 (formerly Family Health International), which sponsored two of the trials included in this review. However, they were not employed at FHI at the time of the trials nor were they involved in the trials.
Figures




Update of
-
Triphasic versus monophasic oral contraceptives for contraception.Cochrane Database Syst Rev. 2006 Jul 19;(3):CD003553. doi: 10.1002/14651858.CD003553.pub2. Cochrane Database Syst Rev. 2006. Update in: Cochrane Database Syst Rev. 2011 Nov 09;(11):CD003553. doi: 10.1002/14651858.CD003553.pub3. PMID: 16856013 Updated.
References
References to studies included in this review
Agoestina 1987 {published data only}
-
- Agoestina T, Sulaeman M, Rarung M, Sabarudin U. Clinical evaluation of low dose pill triphasic (EE + estoden) versus monophasic (EE + desogestrel). Presented at the XIth Asian and Oceanic Congress of Obstetrics and Gynecology; 1987 Dec 6‐12; Hongkong.
Andrade 1993 {published data only}
-
- Andrade RP. Clinical comparison of a triphasic gestodene preparation and a monophasic desogestrel preparation. Gynecological Endocrinology 1993;7 Suppl:33‐41.
Bruni 2000 {published data only}
-
- Bruni V, Croxatto H, Cruz J, Dhont M, Durlot F, Fernandes MT, et al. A comparison of cycle control and effect on well‐being of monophasic gestodene‐, triphasic gestodene‐ and monophasic desogestrel‐containing oral contraceptives. Gynecological Endocrinology 2000;14:90‐8. - PubMed
-
- Lacante P. A comparison of cycle control and effect on well‐being of monophasic gestodene‐, triphasic gestodene‐ and monophasic desogestrel‐containing oral contraceptives. Gynecological Endocrinology 1996;10 Suppl 2:33‐41. - PubMed
Carlborg 1983 {published and unpublished data}
-
- Carlborg L. Acceptability of low‐dose oral contraceptives: results of a randomized Swedish multicenter study comparing a triphasic (Trionetta) and a fixed‐dose combination (Neovletta). Benefits and risk of hormonal contraception: Proceedings of an International Symposium; 1982 March 19; Amsterdam. Boston (MA): MTP Press, 1982:78‐92.
-
- Carlborg L. Comparison of contraceptive acceptability of levonorgestrel and ethinyl oestradiol administered in one three‐phasic (Trionetta) and one monophasic (Neovletta) version. Contraception 1983;27:439‐52. - PubMed
Chavez 1999 {published and unpublished data}
-
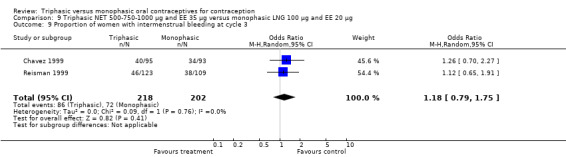
- Chavez A, DelConte A. A comparison of cycle control with monophasic levonorgestrel/ethinylestradiol 100 micrograms/20 micrograms versus triphasic norethindrone/ethinylestradiol 500‐750‐1000 micrograms/35 micrograms: a multicenter, randomized, open‐label study. European Journal of Contraception and Reproductive Health Care 1999;4:75‐83. - PubMed
Chen 1987 {published data only}
-
- Chen JK. A comparative clinical study of the effects of three types of low dose estrogen/progestogen oral contraceptives. Reproduction and Contraception 1987;7:11‐6. - PubMed
-
- Chen JK. A comparative clinical study of the effects of three types of low‐dose estrogen/progestogen oral contraceptives. Shengzhi Yu Biyun 1987;7:11‐6. - PubMed
Dieben 1984 {published and unpublished data}
-
- Cullberg G. A comparative multicentre study on a triphasic, and a fixed low‐dose oral contraceptive combination. Acta Obstetricia et Gynecologica Scandinavica. Supplement 1983;116:97.
-
- Cullberg G, Samsioe G, Andersen RF, Bredesgaard P, Andersen NB, Ernerot H, et al. Two oral contraceptives, efficacy, serum proteins, and lipid metabolism. A comparative multicentre study on a triphasic and a fixed dose combination. Contraception 1982;26:229‐43. - PubMed
-
- Dieben T. A comparative study of the clinical efficacy of Marvelon and a triphasic combination. Organorama 1984;21:16‐8.
-
- Mattsson LA, Cullberg G. Clinical and metabolic effects of Marvelon: Scandinavian experience. British Journal of Family Planning 1984;10:43‐8.
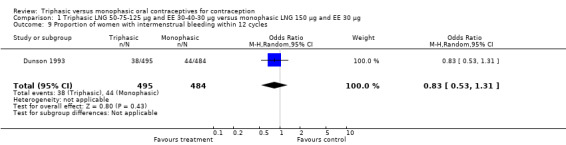
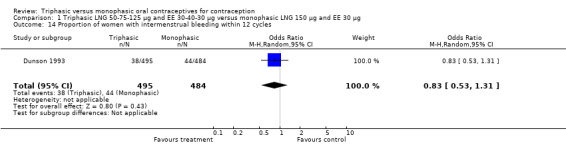
Dunson 1993 {published and unpublished data}
-
- Dunson TR, McLaurin VL, Aguayo EL, Silva P, Calventi V, Gerais AS, et al. A multicenter comparative trial of triphasic and monophasic, low dose combined oral contraceptives. Contraception 1993;47:515‐25. - PubMed
Engebretsen 1987 {published data only}
-
- Engebretsen T, Thorsen E, Smith CC, Bull‐Njaa T, Christensen A. Triphasic versus monophasic p‐pill. A comparative multicenter study [Trefasisk versus monofasisk p‐pille: en sammenlignende multisenterstudie]. Tidsskrift for den Norske Laegeforening 1987;107:941‐3. - PubMed
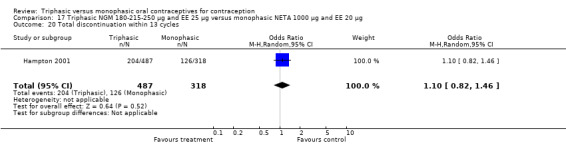
Hampton 2001 {published and unpublished data}
-
- Hampton RM, Fisher AC, Pagano S, LaGuardia KD. Scheduled and unscheduled bleeding patterns with two combined hormonal contraceptives: application of new recommendations for standardization. Fertility and Sterility 2009;92(2):434‐40. - PubMed
-
- Hampton RM, Short M, Bieber E, Bouchard C, Ayotte N, et al. Comparison of a novel norgestimate/ethinyl estradiol oral contraceptive (Ortho Tri‐Cyclen Lo) with the oral contraceptive Loestrin Fe 1/20. Contraception 2001;63:289‐95. - PubMed
-
- Hampton RM, Zhang HF, Barnowski C, Wan GJ. Bleeding patterns with monophasic and triphasic low‐dose ethinyl estradiol combined oral contraceptives. Contraception 2008;77:415‐9. - PubMed
Ismail 1991 {published and unpublished data}
-
- Ismail MTM. A randomised comparative study of Triquilar versus Marvelon: the Malaysian experience. Malaysian Journal of Reproductive Health 1991;9:9‐17. - PubMed
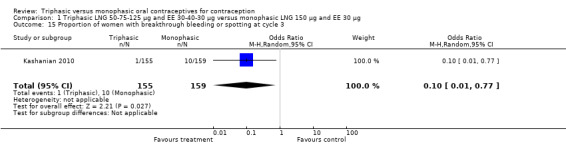
Kashanian 2010 {published data only}
-
- Kashanian M, Shahpourian F, Zare O. A comparison between monophasic levonorgestrel‐ethinyl estradiol 150/30 and triphasic levonorgestrel‐ethinyl estradiol 50‐75‐125/30‐40‐30 contraceptive pills for side effects and patient satisfaction: a study in Iran. European Journal of Obstetrics, Gynecology, and Reproductive Biology. 2010/02/27 2010; Vol. 150, issue 1:47‐51. - PubMed
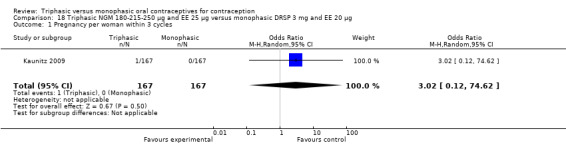
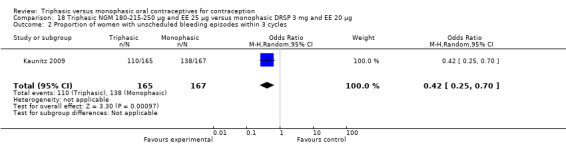
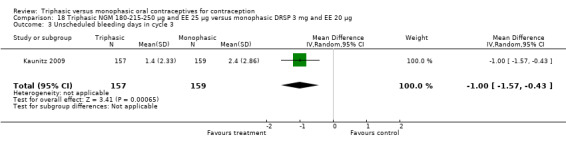
Kaunitz 2009 {published data only}
-
- Kaunitz AM, Burkman RT, Fisher AC, LaGuardia KD. Cycle control with a 21‐day compared with a 24‐day oral contraceptive pill: a randomized controlled trial. Obstetrics & Gynecology. 2009/11/26 2009; Vol. 114, issue 6:1205‐12. - PubMed
Lachnit‐Fixson 1984 {published data only}
-
- Lachnit‐Fixson U. Progress in oral contraception. Advantages of a levonorgestrel‐containing 3‐stage preparation over low‐dose levonorgestrel and desogestrel containing monophasic combination preparations [Fortschritte in der oralen kontrazeption: vorteille eines levonorgestrel‐haltigen dreistufenpraparates gegenuber niedrigdosierten levonorgestrel‐ und desogestrel‐haltigen monophasischen kombinationspraparaten]. Fortschritte der Medizin 1984;102:825‐30. - PubMed
-
- Lachnit‐Fixson U, Aydinlik S, Lehnert J. Clinical comparison between a monophasic preparation and a triphasic preparation. In: Rolland R, Harrison RF, Bonnar J, Thompson W editor(s). Advances in fertility control and the treatment of sterility. Proceedings of a special symposium held at the XIth World Congress on Fertility and Sterility; 1983 June; Dublin. Lancaster: MTP Press, 1984:71‐9.
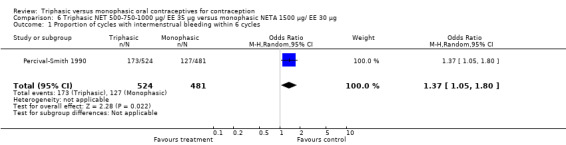
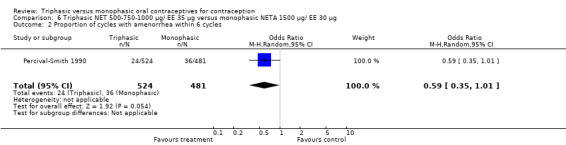
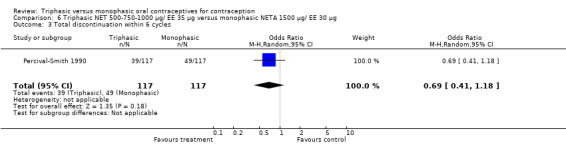
Percival‐Smith 1990 {published data only}
-
- Percival‐Smith RK, Yuzpe AA, Desrosiers JA, Rioux JE, Guilbert E. Cycle control on low‐dose oral contraceptives: a comparative trial. Contraception 1990;42:253‐62. - PubMed
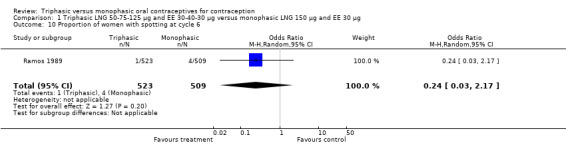
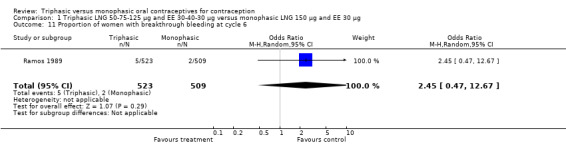
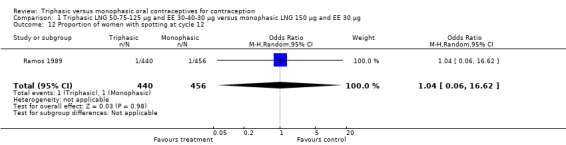
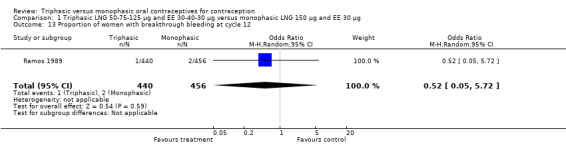
Ramos 1989 {published data only}
-
- Ramos R, Apelo R, Osteria T, Vilar E. A comparative analysis of three different dose combinations of oral contraceptives. Contraception 1989;39:165‐77. - PubMed
Reisman 1999 {published and unpublished data}
-
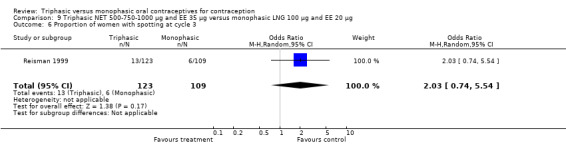
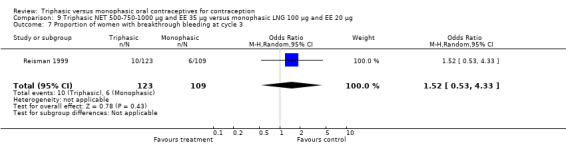
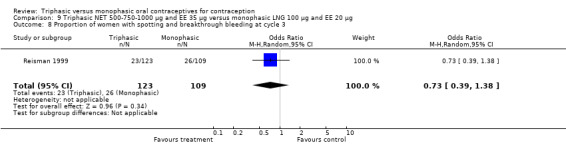
- Reisman H, Martin D, Gast MJ. A multicenter randomized comparison of cycle control and laboratory findings with oral contraceptive agents containing 100 μg levonorgestrel with 20 μg ethinyl estradiol or triphasic norethindrone with ethinyl estradiol. American Journal of Obstetrics and Gynecology 1999;181:45‐52. - PubMed
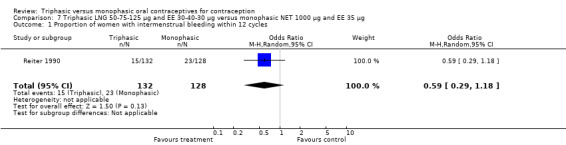
Reiter 1990 {published and unpublished data}
-
- Reiter SL, Baer LJ. Initial selection of oral contraceptives. Journal of Reproductive Medicine 1990;35:547‐8. - PubMed
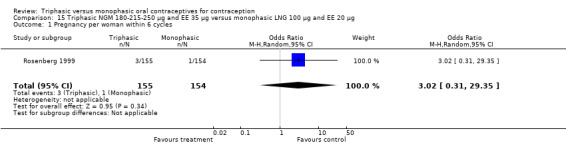
Rosenberg 1999 {published and unpublished data}
-
- Rosenberg MJ, Meyers A, Roy V. Efficacy, cycle control, and side effects of low‐ and lower‐dose oral contraceptives: a randomized trial of 20 μg and 35 μg estrogen preperations. Contraception 1999;60:321‐9. - PubMed
Rowan 1999 {published and unpublished data}
-
- Rowan JP. "Estrophasic" dosing: A new concept in oral contraceptive therapy. American Journal of Obstetrics and Gynecology 1999;180:302‐6. - PubMed
Saxena 1992 {published and unpublished data}
-
- Datey S, Gaur LN, Saxena BN. Vaginal bleeding patterns of women using different contraceptive methods (implants, injectables, IUDs, oral pills)‐an Indian experience. Contraception 1995;51:155‐65. - PubMed
-
- Saxena B. Randomised clinical trial with Triquilar‐ED and low‐dose combination pill. Journal of Obstetrics and Gynaecology of India 1992;42:71‐7.
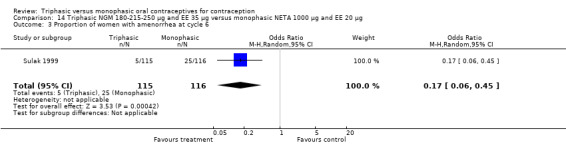
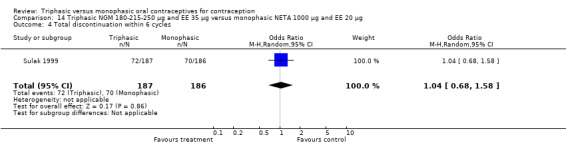
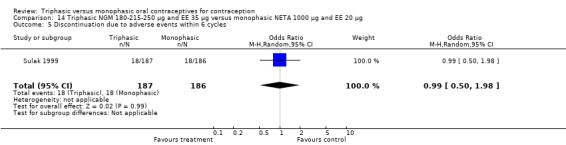
Sulak 1999 {published data only}
-
- Lippman J, Siu C, Godwin A, Massaro J. A clinical comparison of two oral contraceptives: triphasic norgestimate/35 μg ethinylestradiol versus monophasic norethindrone acetate/20 μg ethinylestradiol. Obstetrics & Gynecology 1999;93 Suppl:37.
-
- Sulak P, Lippman J, Siu C, Massaro J, Godwin A. Clinical comparison of triphasic norgestimate/35 μg ethinyl estradiol and monophasic norethindrone acetate/20 μg ethinyl estradiol: cycle control, lipid effects, and user satisfaction. Contraception 1999;59:161‐6. - PubMed
Zador 1979 {published data only}
-
- Lachnit‐Fixson U. Clinical investigation with a new triphasic oral contraceptive. In: Greenblatt RB editor(s). The development of a new triphasic oral contraceptive. Proceedings of a Special Symposium held at the 10th World Congress on Fertility and Sterility; 1980 July; Madrid. Lancaster: MTP Press Limited, 1980:99‐107.
-
- Lachnit‐Fixson U. Progress in oral contraception. Advantages of a levonorgestrel‐containing 3‐stage preparation over low‐dose levonorgestrel and desogestrel containing monophasic combination preparations [Fortschritte in der oralen kontrazeption: vorteille eines levonorgestrel‐haltigen dreistufenpraparates gegenuber niedrigdosierten levonorgestrel‐ und desogestrel‐haltigen monophasischen kombinationspraparaten]. Fortschritte der Medizin 1984;102:825‐30. - PubMed
-
- Lachnit‐Fixson U. The first three‐stage preparation for hormonal contraception. Clinical results [Erstes dreistufenpraeparat zur hormonalen konzeptionsverhutung: klinische ergebnisse]. Munchener Medizinische Wochenschrift 1979;121:1421‐6. - PubMed
-
- Zador G. Clinical performance of a triphasic administration of ethinyl estradiol and levonorgestrel in comparison with the 30 + 150 μg fixed‐dose regimen. In: Haspels AA, Rolland R editor(s). Benefits and risk of hormonal contraception. Proceedings of an international symposium; 1982 March 19; Amsterdam. Boston (Massachusetts): MTP Press, 1982:43‐55.
-
- Zador G. Fertility regulation using "triphasic" administration of ethinyl estradiol and levonorgestrel in comparison with the 30 plus 150 μg fixed dose regime. Acta Obstetricia et Gynecologica Scandinavica. Supplement 1979;88:43‐8. - PubMed
References to studies excluded from this review
Bancroft 1987 {published data only}
-
- Bancroft J, Sanders D, Warner P, Loudon N. The effects of oral contraceptives on mood and sexuality: A comparison of triphasic and combined preparations. Journal of Psychosomatic Obstetrics and Gynaecology 1987;7:1‐8.
Christie 1989 {published data only}
-
- Christie T. A clinical overview of a new triphasic contraceptive containing gestodene. International Journal of Fertility 1989;34 Suppl:40‐9. - PubMed
Dik 1984 {published data only}
-
- Dik M, Eckert H, Hones S, Schindler AE. Comparison of a 2‐phase preparation (Oviol 22) with a low‐dose 1‐phase preparation (Ovoresta M) [Vergleich eines zweiphasenpraparates (Oviol 22) mit einem niedrig dosierten Einphasenpraparat (Ovoresta M)]. Geburtshilfe und Frauenheilkunde 1984;44:808‐12. - PubMed
Dubnitskaia 1988 {published data only}
-
- Dubnitskaia LV. Acceptability of hormonal contraceptives with a low steroid content. Akusherstvo I Ginekologiia 1988;8:47‐50. - PubMed
Grace 1994 {published data only}
-
- Grace E, Emans SJ, Havens KK, Merola JL, Woods ER. Contraceptive compliance with a triphasic and a monophasic norethindrone‐containing oral contraceptive pill in a private adolescent practice. Adolescent and Pediatric Gynecology 1994;7:29‐33.
Kuhl 1985 {published data only}
-
- Kuhl H, Gahn G, Romberg G, Marz W, Taubert H‐D. A randomized cross‐over comparison of two low‐dose oral contraceptives upon hormonal and metabolic parameters: 1. Effects upon sexual hormone levels. Contraception 1985;31:583‐93. - PubMed
Matsumoto 1988 {published data only}
-
- Matsumoto S, Sato T, Matsuyama E, Tamada T, Wagatsuma T, Honda H. Results of a clinical study with low‐dose oral contraceptives: investigation with triphasic and monophasic preparations containing levonorgestrel and ethinylestradiol. Current Therapeutic Research, Clinical and Experimental 1988;44:165‐77.
Otolorin 1989 {published data only}
-
- Otolorin EO. Clinical experience with a triphasic oral contraceptive containing ethinyloestradiol and levonorgestrel in Nigerian women. West African Journal of Medicine 1989;8:116‐21. - PubMed
Perrone 1987 {published data only}
-
- Perrone G, Calzolari E, Mancone M, Masci A, Steffe M, Tesseri E. Oral contraceptives and their minor side effects: comparison of three low‐dose estroprogestinic combinations [Contraccettivi orali ed effetti collaterali minori: confronto fra tre estroprogestinici a basso dosaggio]. Patologia e Clinica Ostetrica e Ginecologica 1987;15:6‐11. - PubMed
Rubio‐Lotvin 1992 {published data only}
-
- Rubio‐Lotvin B, Ruiz‐Moreno JA, Gonzalez‐Ansorena R. Desogestrel‐ethinylestradiol, an oral monophasic contraceptive. Clinical and lipid metabolic effects: a 5 year experience. Advances in Contraceptive Delivery Systems 1992;8:75‐88. - PubMed
References to ongoing studies
Bayer 2011 {unpublished data only}
-
- Bayer Schering Pharma AG. Cycle Control and Safety of E2‐DRSP. Available from: http://clinicaltrials.gov/ct2/home (accessed 04 May 2011). [NCT00653614]
Additional references
Als‐Nielsen 2003
-
- Als‐Nielsen B, Chen W, Gluud C, Kjaergard LL. Association of funding and conclusions in randomized drug trials: a reflection of treatment effect or adverse events?. JAMA 2003;290:921‐8. - PubMed
Belsey 1986
-
- Belsey EM, Machin D, d' Arcangues C. The analysis of vaginal bleeding patterns induced by fertility regulating methods. World Health Organization Special Programme of Research, Development and Research Training in Human Reproduction. Contraception 1986;34:253‐61. - PubMed
Berlin 1997
-
- Berlin JA. Does blinding of readers affect the results of meta‐analyses?. Lancet 1997;350:185‐6. - PubMed
CONSORT 2010
-
- CONSORT group. CONSORT: Transparent reporting of trials. http://www.consort‐statement.org/ (accessed 04 May 2011).
DerSimonian 1982
-
- DerSimonian R, Charette LJ, McPeek B, Mosteller F. Reporting on methods in clinical trials. New England Journal of Medicine 1982;306:1332‐7. - PubMed
Fay 1982
Gallo 2008
Graham 1982
Guillebaud 1993
-
- Guillebaud J. Contraception: your questions answered. 2nd Edition. Edinburgh: Churchill Livingstone, 1993:188‐90.
Hale 1987
-
- Hale RW. Phasic approach to oral contraceptives. American Journal of Obstetrics and Gynecology 1987;157:1052‐8. - PubMed
Higgins 2005
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions 4.2.5 [updated May 2005]. In: The Cochrane Library 2005, Issue 3. Chichester, UK: John Wiley & Sons, Ltd. Chicester, UK: John Wiley & Sons, Ltd.
IPPF 2004
-
- Terki F, Malhotra U. In: Powlson M editor(s). Medical and Service Delivery Guidelines for Sexual and Reproductive Health Services. Third Edition. London (UK): International Planned Parenthood Federation, 2004.
Juni 1999
-
- Juni P, Witschi A, Bloch R, Egger M. The hazards of scoring the quality of clinical trials for meta‐analysis. JAMA 1999;282:1054‐60. - PubMed
Ketting 1988
-
- Ketting, E. The relative reliability of oral contraceptives: findings of an epidemiological study. Contraception 1988;37:343‐8. - PubMed
Kovacs 1989
-
- Kovacs, GT, Riddoch G, Duncombe P, Welberry L, Chick P, et al. Inadvertent pregnancies in oral contraceptive users. Medical Journal of Australia 1989;150:549‐51. - PubMed
Lexchin 2003
Maitra 2004
Mishell 2007
-
- Mishell DR, Guillebaud J, Westhoff C, Nelson AL, Kaunitz AM, Trussell J, et al. Recommendations for standardization of data collection and analysis of bleeding in combined hormone contraceptive trials. Contraception 2007;75(1):11‐5. - PubMed
Moreau 2007
-
- Moreau C, Trussell J, Gilbert F, Bajos N, Bouyer J. Oral contraceptive tolerance. Does the type of pill matter?. Obstetrics & Gynecology 2007;109:1277‐85. - PubMed
Rosenberg 1992
-
- Rosenberg MJ, Long SC. Oral contraceptives and cycle control: a critical review of the literature. Advances in Contraception 1992;8 Suppl:35‐45. - PubMed
Rosenberg 1995
-
- Rosenberg MJ, Waugh MS, Meehan TE. Use and misuse of oral contraceptives: risk indicators for poor pill taking and discontinuation. Contraception 1995;51:283‐8. - PubMed
Rosenberg 1998
-
- Rosenberg MJ, Waugh MS. Oral contraceptive discontinuation: a prospective evaluation of frequency and reasons. American Journal of Obstetrics and Gynecology 1998;179:577‐82. - PubMed
Schulz 2002a
-
- Schulz KF, Grimes DA. Sample size slippages in randomised trials: exclusions and the lost and wayward. Lancet 2002;359:781‐5. - PubMed
Schulz 2002b
-
- Schulz KF, Chalmers I, Altman DG. The landscape and lexicon of blinding in randomized trials. Annals of Internal Medicine 2002;136:254‐9. - PubMed
Schulz 2002c
-
- Schulz KF, Grimes DA. Generation of allocation sequences in randomised trials: chance, not choice. Lancet 2002;359:515‐9. - PubMed
Schulz 2002d
-
- Schulz KF, Grimes DA. Allocation concealment in randomised trials: defending against deciphering. Lancet 2002;359:614‐8. - PubMed
Schulz 2002e
-
- Schulz KF, Grimes DA. Blinding in randomised trials: hiding who got what. Lancet 2002;359:696‐700. - PubMed
Strauss 2005
-
- Strauss SE, Richardson WS, Glasziou P, Haynes RB. Evidence‐based Medicine: How to Practice and Teach EBM. Third Edition. New York: Churchill Livingstone, 2005.
Trussell 1991
-
- Trussell J. Methodological pitfalls in the analysis of contraceptive failure. Statistics in Medicine 1991;10:201‐20. - PubMed
Upton 1983
-
- Upton GV. The phasic approach to oral contraception:the triphasic concept and its clinical application. International Journal of Fertility 1983;28:121‐40. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical