

Clotting factor deficiency in early trauma-associated coagulopathy
- PMID: 22071999
- PMCID: PMC3241929
- DOI: 10.1097/TA.0b013e318232e5ab
Clotting factor deficiency in early trauma-associated coagulopathy
Abstract
Background: Coagulopathic bleeding is a leading cause of in-hospital death after injury. A recently proposed transfusion strategy calls for early and aggressive frozen plasma transfusion to bleeding trauma patients, thus addressing trauma-associated coagulopathy (TAC) by transfusing clotting factors (CFs). This strategy may dramatically improve survival of bleeding trauma patients. However, other studies suggest that early TAC occurs by protein C activation and is independent of CF deficiency. This study investigated whether CF deficiency is associated with early TAC.
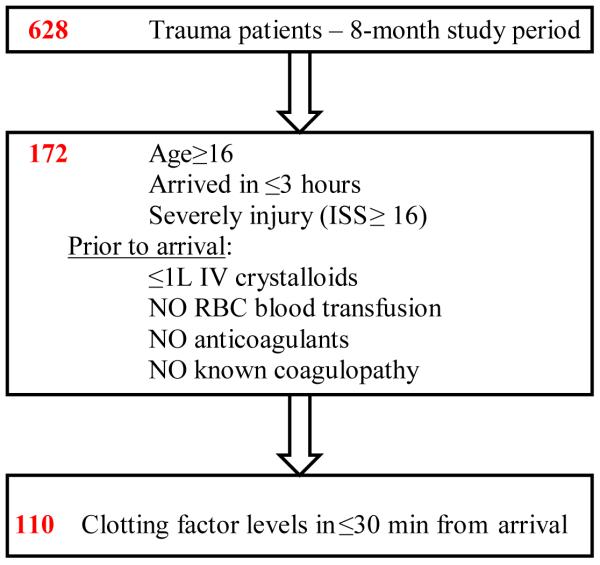
Methods: This is a prospective observational cohort study of severely traumatized patients (Injury Severity Score ≥ 16) admitted shortly after injury, receiving minimal fluids and no prehospital blood. Blood was assayed for CF levels, thromboelastography, and routine coagulation tests. Critical CF deficiency was defined as ≤ 30% activity of any CF.
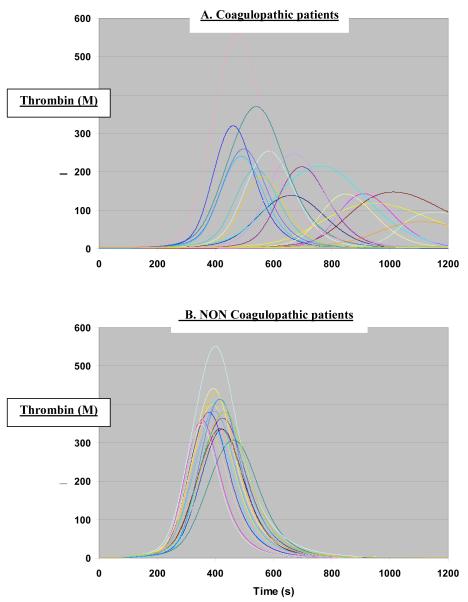
Results: Of 110 patients, 22 (20%) had critical CF deficiency: critically low factor V level was evident in all these patients. International normalized ratio, activated prothrombin time, and, thromboelastography were abnormal in 32%, 36%, and 35%, respectively, of patients with any critically low CF. Patients with critical CF deficiency suffered more severe injuries, were more acidotic, received more blood transfusions, and showed a trend toward higher mortality (32% vs. 18%, p = 0.23). Computational modeling showed coagulopathic patients had pronounced delays and quantitative deficits in generating thrombin.
Conclusions: Twenty percent of all severely injured patients had critical CF deficiency on admission, particularly of factor V. The observed factor V deficit aligns with current understanding of the mechanisms underlying early TAC. Critical deficiency of factor V impairs thrombin generation and profoundly affects hemostasis.
Figures
References
-
- Hoyt DB, Bulger EM, Knudson MM, et al. Death in the operating room: an analysis of a multicenter experience. J Trauma. 1994;37:426–432. - PubMed
-
- Tien HC, Spencer F, Tremblay LN, et al. Preventable deaths from hemorrhage at a level I Canadian trauma center. J Trauma. 2007;62:142–146. - PubMed
-
- Holcomb JB, Wade CE, Michalek JE, et al. Increased plasma and platelet to red blood cell ratios improves outcome in 466 massively transfused civilian trauma patients. Ann Surg. 2008;248:447–458. - PubMed
-
- Hess JR, Brohi K, Dutton RP, et al. The coagulopathy of trauma: a review of mechanisms. J Trauma. 2008;65:748–754. - PubMed
-
- Lasne D, Jude B, Susen S. From normal to pathological hemostasis. Can J Anaesth. 2006;53:S2–11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
