

Real-time functional magnetic resonance imaging neurofeedback for treatment of Parkinson's disease
- PMID: 22072682
- PMCID: PMC6633236
- DOI: 10.1523/JNEUROSCI.3498-11.2011
Real-time functional magnetic resonance imaging neurofeedback for treatment of Parkinson's disease
Abstract
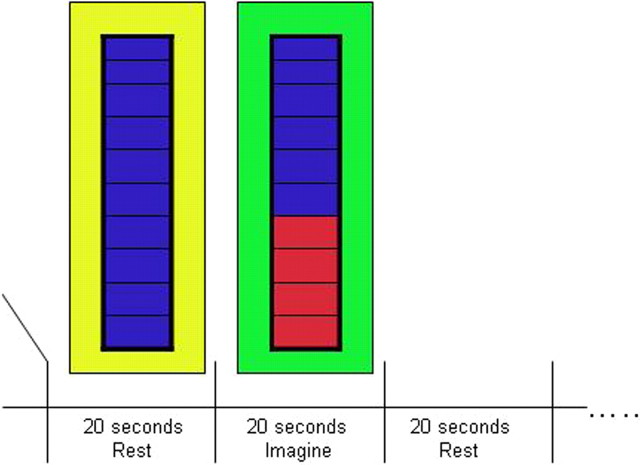
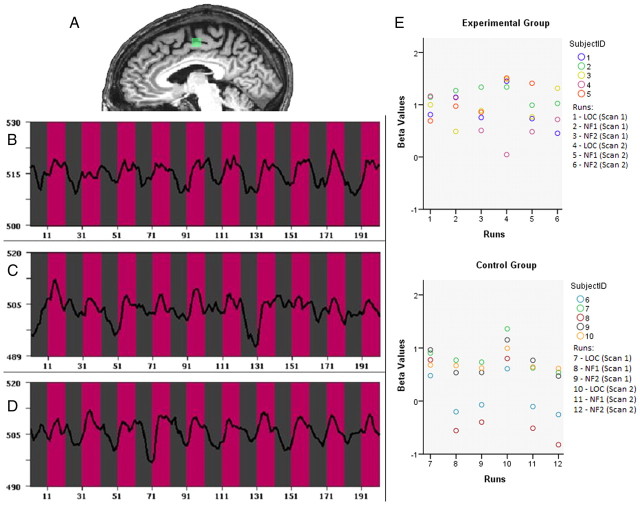
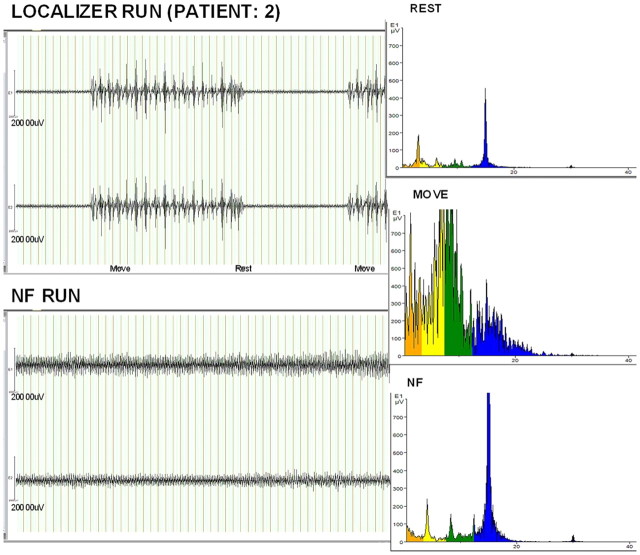
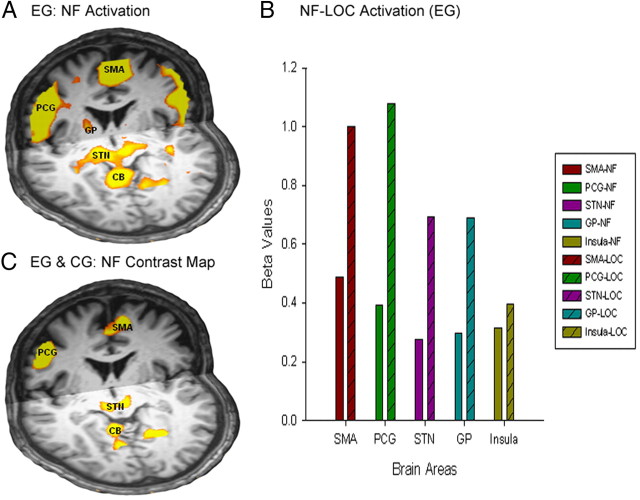
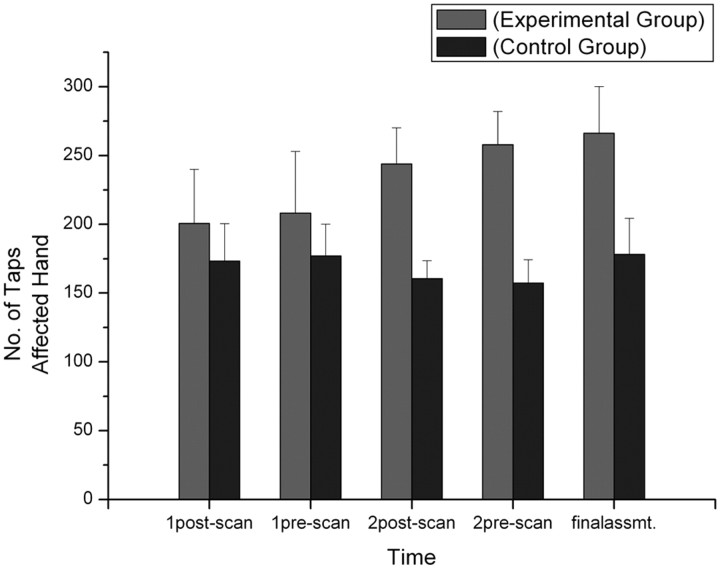
Self-regulation of brain activity in humans based on real-time feedback of functional magnetic resonance imaging (fMRI) signal is emerging as a potentially powerful, new technique. Here, we assessed whether patients with Parkinson's disease (PD) are able to alter local brain activity to improve motor function. Five patients learned to increase activity in the supplementary motor complex over two fMRI sessions using motor imagery. They attained as much activation in this target brain region as during a localizer procedure with overt movements. Concomitantly, they showed an improvement in motor speed (finger tapping) and clinical ratings of motor symptoms (37% improvement of the motor scale of the Unified Parkinson's Disease Rating Scale). Activation during neurofeedback was also observed in other cortical motor areas and the basal ganglia, including the subthalamic nucleus and globus pallidus, which are connected to the supplementary motor area (SMA) and crucial nodes in the pathophysiology of PD. A PD control group of five patients, matched for clinical severity and medication, underwent the same procedure but did not receive feedback about their SMA activity. This group attained no control of SMA activation and showed no motor improvement. These findings demonstrate that self-modulation of cortico-subcortical motor circuits can be achieved by PD patients through neurofeedback and may result in clinical benefits that are not attainable by motor imagery alone.
Figures
Similar articles
-
Resting-state functional magnetic resonance imaging of the subthalamic microlesion and stimulation effects in Parkinson's disease: Indications of a principal role of the brainstem.Neuroimage Clin. 2015 Aug 21;9:264-74. doi: 10.1016/j.nicl.2015.08.008. eCollection 2015. Neuroimage Clin. 2015. PMID: 26509113 Free PMC article.
-
Beta-band oscillations in the supplementary motor cortex are modulated by levodopa and associated with functional activity in the basal ganglia.Neuroimage Clin. 2018 May 18;19:559-571. doi: 10.1016/j.nicl.2018.05.021. eCollection 2018. Neuroimage Clin. 2018. PMID: 29984164 Free PMC article.
-
Increased SMA-M1 coherence in Parkinson's disease - Pathophysiology or compensation?Exp Neurol. 2013 Sep;247:178-81. doi: 10.1016/j.expneurol.2013.04.013. Epub 2013 May 9. Exp Neurol. 2013. PMID: 23664959
-
Towards therapeutic electrophysiological neurofeedback in Parkinson's disease.Parkinsonism Relat Disord. 2024 Apr;121:106010. doi: 10.1016/j.parkreldis.2024.106010. Epub 2024 Jan 14. Parkinsonism Relat Disord. 2024. PMID: 38245382 Review.
-
Real-time functional magnetic resonance imaging neurofeedback in motor neurorehabilitation.Curr Opin Neurol. 2016 Aug;29(4):412-8. doi: 10.1097/WCO.0000000000000340. Curr Opin Neurol. 2016. PMID: 27213774 Free PMC article. Review.
Cited by
-
Combining Real-Time fMRI Neurofeedback Training of the DLPFC with N-Back Practice Results in Neuroplastic Effects Confined to the Neurofeedback Target Region.Front Behav Neurosci. 2016 Jun 28;10:138. doi: 10.3389/fnbeh.2016.00138. eCollection 2016. Front Behav Neurosci. 2016. PMID: 27445733 Free PMC article.
-
Self-Regulation of Blood Oxygenation Level Dependent Response: Primary Effect or Epiphenomenon?Front Neurosci. 2016 Mar 24;10:117. doi: 10.3389/fnins.2016.00117. eCollection 2016. Front Neurosci. 2016. PMID: 27047332 Free PMC article. No abstract available.
-
How feedback, motor imagery, and reward influence brain self-regulation using real-time fMRI.Hum Brain Mapp. 2016 Sep;37(9):3153-71. doi: 10.1002/hbm.23228. Epub 2016 Jun 6. Hum Brain Mapp. 2016. PMID: 27272616 Free PMC article.
-
Dynamic Functional Network Connectivity Changes Associated with fMRI Neurofeedback of Right Premotor Cortex.Brain Sci. 2021 Apr 30;11(5):582. doi: 10.3390/brainsci11050582. Brain Sci. 2021. PMID: 33946251 Free PMC article.
-
Making sense of real-time functional magnetic resonance imaging (rtfMRI) and rtfMRI neurofeedback.Int J Neuropsychopharmacol. 2015 Feb 25;18(6):pyv020. doi: 10.1093/ijnp/pyv020. Int J Neuropsychopharmacol. 2015. PMID: 25716778 Free PMC article. Review.
References
-
- Albin RL, Young AB, Penney JB. The functional anatomy of basal ganglia disorders. Trends Neurosci. 1989;12:366–375. - PubMed
-
- Beauregard M, Lévesque J. Functional magnetic resonance imaging investigation of the effects of neurofeedback training on the neural bases of selective attention and response inhibition in children with attention-deficit/hyperactivity disorder. Appl Psychophysiol Biofeedback. 2006;31:3–20. - PubMed
-
- Boggio PS, Ferrucci R, Rigonatti SP, Covre P, Nitsche M, Pascual-Leone A, Fregni F. Effects of transcranial direct current stimulation on working memory in patients with Parkinson's disease. J Neurol Sci. 2006;249:31–38. - PubMed
-
- Caria A, Sitaram R, Veit R, Begliomini C, Birbaumer N. Volitional control of anterior insula activity modulates the response to aversive stimuli. A real-time functional magnetic resonance imaging study. Biol Psychiatry. 2010;68:425–432. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical