

Diagnostic and therapeutic-restorative procedures for masticatory dysfunctions
- PMID: 22073067
- PMCID: PMC3201006
Diagnostic and therapeutic-restorative procedures for masticatory dysfunctions
Abstract
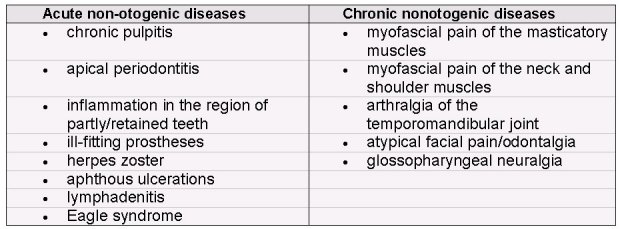
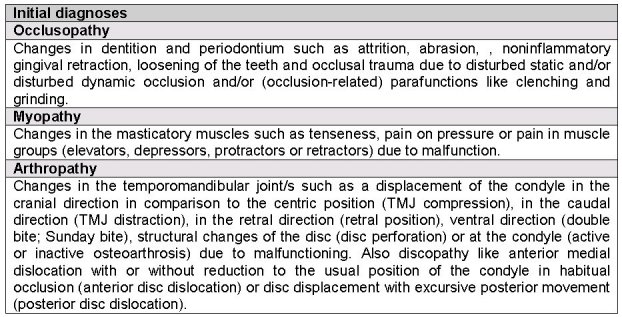
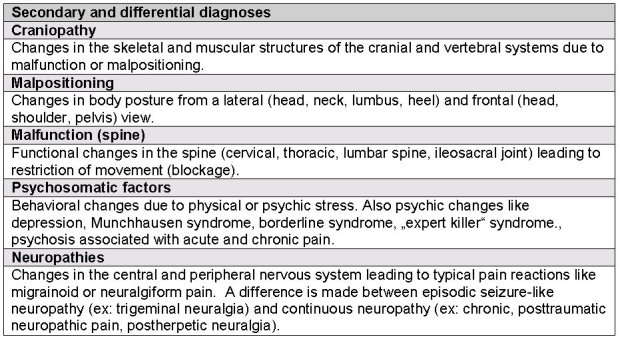
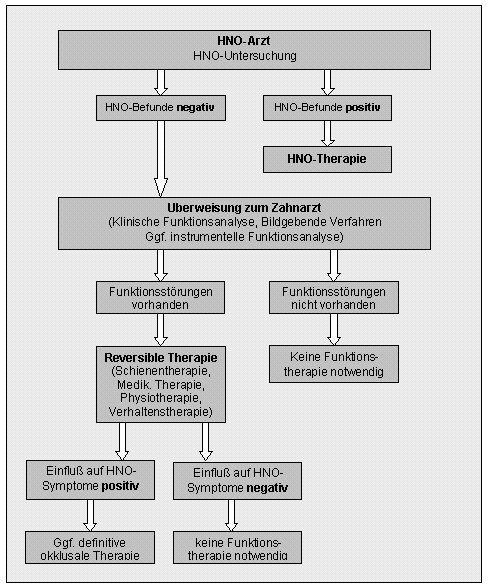
Temporomandibular disorders (TMD) or craniomandibular disorders, respectively, involve diseases of the teeth and periodontia as well as the masticatory muscles, temporomandibular joints and associated structures. It has been shown in recent years that psychological, social and general medical influences are of enormous importance in the etiology of TMD in addition to anatomical, physiological, parafunctional and other biological causes. This signifies that therapists confronted with TMD should already include at an early stage other specialists such as pain therapists, neurologists, ENT physicians, psychotherapists and physiotherapists. Patients need to be referred to dentists specializing in TMD when ENT examinations yield no pathological findings. The treatment of TMD is subdivided into the following steps that are always related to underlying diagnoses: informing patients, self-observation, relaxation therapy, behavioral therapy, physiotherapy, drug therapy, therapeutic local anesthesia, splint therapy, and, if necessary, prosthetic and/or orthodontic therapy to restore a stable occlusion.
Keywords: biopsychosocial disease; functional diagnostics; functional therapy; temporomandibular disorders; tinnitus.
Figures




















References
-
- Türp JC, John M, Nilges P, Jürgens J, Ahlers MO, Böhner M, Busche E, Hugger A, Jakstat HA, Koch WH, Niederfeilner J, Paak S, Palatka P, Peschen-Rosin R, Schindler HJ, Sommer C, Sprotte G, Weißmann K, Wernze H. Schmerzen im Bereich der Kaumuskulatur und Kiefergelenke. Der Schmerz. 2000;14:416–427. - PubMed
-
- Palla S. Grundsätze zur Therapie des myoarthropathischen Schmerzes. Der Schmerz. 2002;16:373–380. - PubMed
-
- Travell JG, Simons DG. Myofascial pain and dysfunction. The Trigger Point Manual. The upper Extremities. Baltimore: Williams & Wilkins; 1983.
-
- Bernhardt O, et al. Signs of temporomandibular disorders in tinnitus patients and in a population-based group of volunteers: results of the Study of Health in Pomerania. J Oral Rehab. 2004;31:311–319. - PubMed
-
- Williamson EH. Interrelationship of internal derangement of the temporomandibular joint, headache, vertigo and tinnitus: a survey of 25 patients. Cranio. 1990;8(4):301–306. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous