

Biomaterials in skull base surgery
- PMID: 22073100
- PMCID: PMC3199810
- DOI: 10.3205/cto000059
Biomaterials in skull base surgery
Abstract
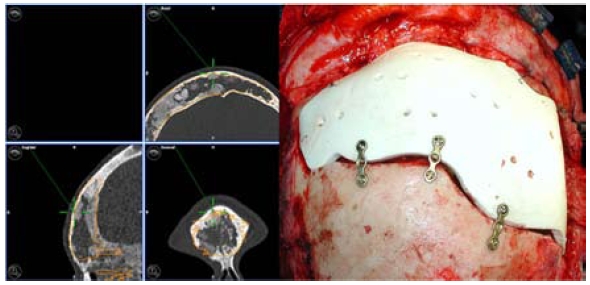
Reconstruction materials and techniques for the base of the skull have undergone rapid developments and differentiation in recent years. While mostly autotransplants, collagens or resorbable alloplastic materials are preferred for duraplasties, pronounced organ-specific differences can be observed in the reconstruction of hard tissues. The use of polymethylmethacryl bone cement, once wide-spread, has decreased greatly due to the release of toxic monomers. Bony autotransplants are still used primarily for smaller skull-base defects, intraoperatively formable titanium nets may be also used for larger fronto- or laterobasal reconstructions of bony defects. Defects in visible areas are increasingly closed with preformed titanium or ceramic implants, which are planned and fitted to the individual patient using preoperative CT imaging. At the skull base, this applies especially to reconstructions of the frontal sinus. For extensive reconstructions of the orbita, titanium nets and non-resorbable plastics have proven valuable; in closing smaller defects especially of the orbital floor, resorbable implants based on Polyglactin 901 are also used.
Keywords: computer assisted surgery; orbital reconstruction; prefabrication; skull base reconstruction.
Figures







References
-
- Potter JK, Ellis E. Biomaterials for the reconstruction of the internal orbit. J Oral Maxillofac Surg. 2004;62:1280–1297. doi: 10.1016/j.joms.2004.04.018. Available from: http://dx.doi.org/10.1016/j.joms.2004.04.018. - DOI - DOI - PubMed
-
- Castelnouvo PG, Delu G, Locatelli D, Padoan G, de Bernardi F, Pistochini A, Bignami M. Endonasal endoscopic duraplasty: Our experience. Skull Base. 2006;16:19–23. doi: 10.1055/s-2005-922096. Available from: http://dx.doi.org/10.1055/s-2005-922096. - DOI - DOI - PMC - PubMed
-
- Aletsee C, Konopik V, Dazert S, Dieler R. Operative Versorgung von Verletzungen der Rhinobasis. Laryngo-Rhino-Otol. 2003;82:626–631. doi: 10.1055/s-2003-42688. Available from: http://dx.doi.org/10.1055/s-2003-42688. - DOI - DOI - PubMed
-
- Draf W, Schick B. How I do it: Endoscopic-microscopic anterior skull base reconstruction. Skull Base. 2007;17:53–58. doi: 10.1055/s-2006-959335. Available from: http://dx.doi.org/10.1055/s-2006-959335. - DOI - DOI - PMC - PubMed
-
- Schick B, Ibing R, Brors D, Draf W. Longterm study in endonasal duraplasty and review of the literature. Ann Otol Laryngol Rhinol. 2001;114:142–147. - PubMed
LinkOut - more resources
Full Text Sources
