

Surgery of the turbinates and "empty nose" syndrome
- PMID: 22073107
- PMCID: PMC3199827
- DOI: 10.3205/cto000067
Surgery of the turbinates and "empty nose" syndrome
Abstract
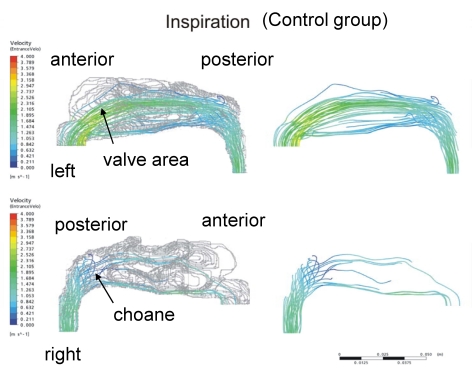
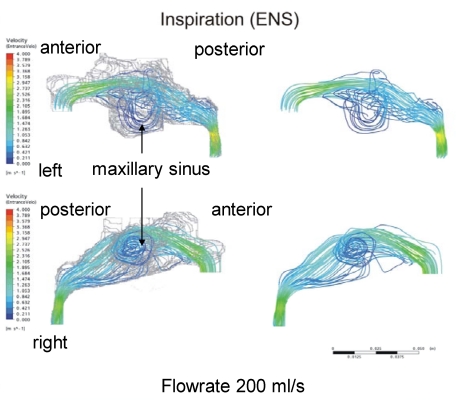
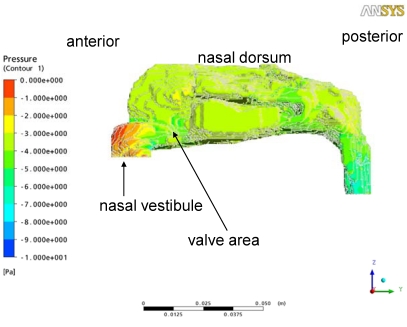
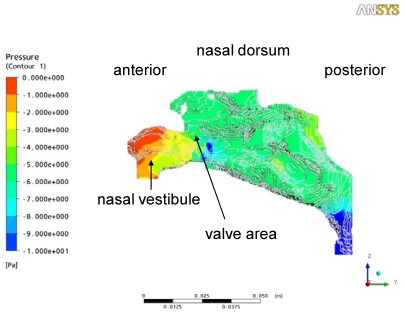
Surgical therapy of the inferior and/or middle turbinate is indicated when conservative treatment options have failed. The desired goal is a reduction of the soft tissue volume of the turbinates regarding the individual anatomic findings, whilst simultaneously conserving as much mucosa as possible. As the turbinates serve as a functional entity within the nose, they ensure climatisation, humidification and cleaning of the inhaled air. Thus free nasal breathing means a decent quality of life, as well.Regarding the multitude of different surgical techniques, we confirm that no ideal standard technique for turbinate reduction has been developed so far. Moreover, there is a lack of prospective and comparable long-term studies, which makes it difficult to recommend evidence-based surgical techniques. However, the anterior turbinoplasty seems to fulfil the preconditions of limited tissue reduction and mucosa-preservation, and therefore it is the method of choice today.Radical resection of the turbinates may lead to severe functional disturbances developing a secondary atrophic rhinitis. The "empty nose" syndrome is a specific entity within the secondary atrophic rhinitis where intranasal changes in airflow result in disturbed climatisation and also interfere with pulmonary function. Results deriving from an actual in vivo study of climatisation and airflow in "empty nose" patients are presented.
Keywords: inferior turbinate; laser surgery; middle turbinate; pediatric surgery of turbinates; turbinate surgery; “empty nose” syndrome.
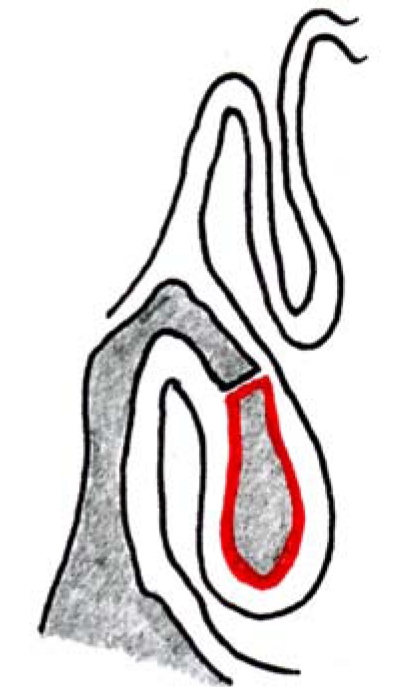
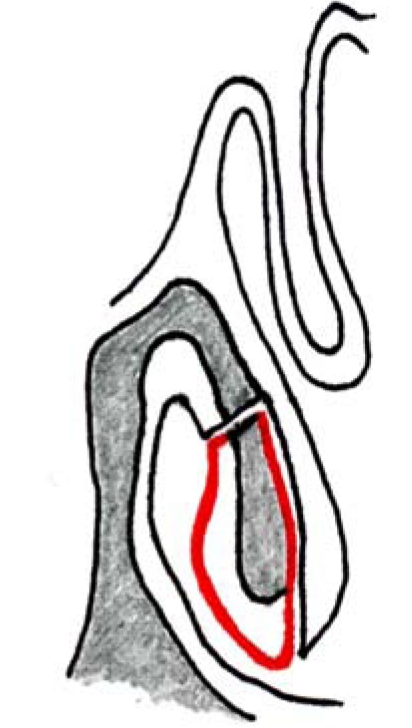
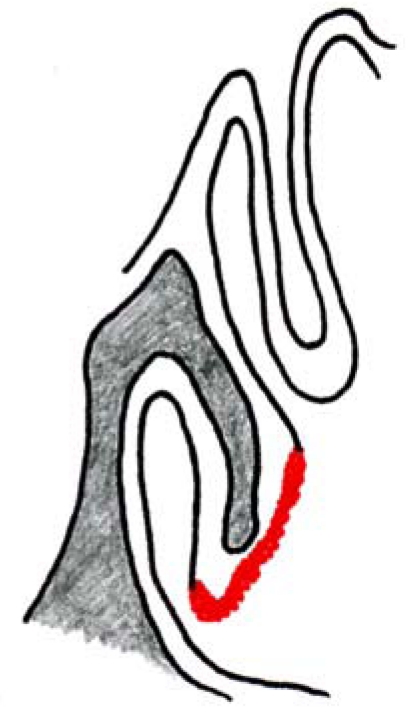
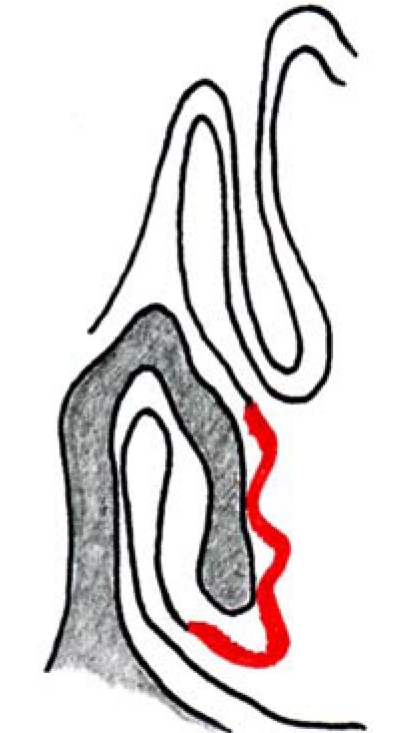
Figures
References
-
- Tasman AJ. Die untere Nasenmuschel: Dysregulation und chirurgische Verkleinerung. Laryngo-Rhino-Otol. 2002;81:822–833. doi: 10.1055/s-2002-35772. Available from: http://dx.doi.org/10.1055/s-2002-35772. - DOI - PubMed
-
- Juniper EF. Impact of upper respiratory allergic diseases on quality of life. J Allergy Clin Immunol. 1998;101(suppl):386–391. doi: 10.1016/S0091-6749(98)70227-1. Available from: http://dx.doi.org/10.1016/S0091-6749(98)70227-1. - DOI - PubMed
-
- Kayser R. Die exakte Messung der Luftdurchgängigkeit der Nase. Arch Laryng Rhinol (Berl) 1895;8:101.
-
- Eccles R. A role for the nasal cycle in respiratory defence. Eur Repir J. 1996;9(2):371–376. doi: 10.1183/09031936.96.09020371. Available from: http://dx.doi.org/10.1183/09031936.96.09020371. - DOI - PubMed
-
- Maran AGD, Lund VJ. Nasal Physiology. In: Maran AGD, Lund VJ, editors. Clinical Rhinology. Stuttgart: Thieme; 1990. p. 5.
LinkOut - more resources
Full Text Sources
