

Time to recurrence and survival in serous ovarian tumors predicted from integrated genomic profiles
- PMID: 22073136
- PMCID: PMC3207809
- DOI: 10.1371/journal.pone.0024709
Time to recurrence and survival in serous ovarian tumors predicted from integrated genomic profiles
Abstract
Background: Serous ovarian cancer (SeOvCa) is an aggressive disease with differential and often inadequate therapeutic outcome after standard treatment. The Cancer Genome Atlas (TCGA) has provided rich molecular and genetic profiles from hundreds of primary surgical samples. These profiles confirm mutations of TP53 in ~100% of patients and an extraordinarily complex profile of DNA copy number changes with considerable patient-to-patient diversity. This raises the joint challenge of exploiting all new available datasets and reducing their confounding complexity for the purpose of predicting clinical outcomes and identifying disease relevant pathway alterations. We therefore set out to use multi-data type genomic profiles (mRNA, DNA methylation, DNA copy-number alteration and microRNA) available from TCGA to identify prognostic signatures for the prediction of progression-free survival (PFS) and overall survival (OS).
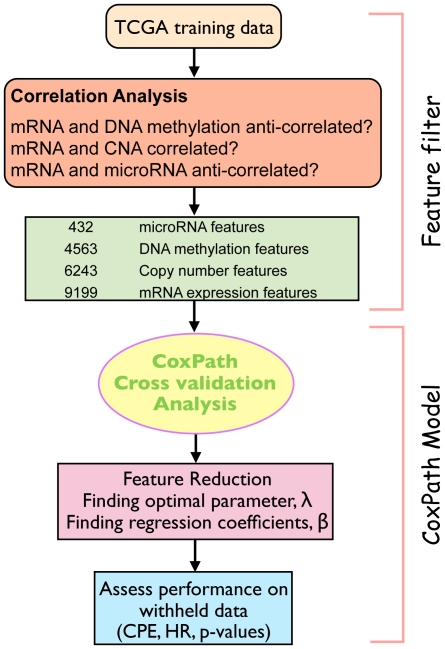
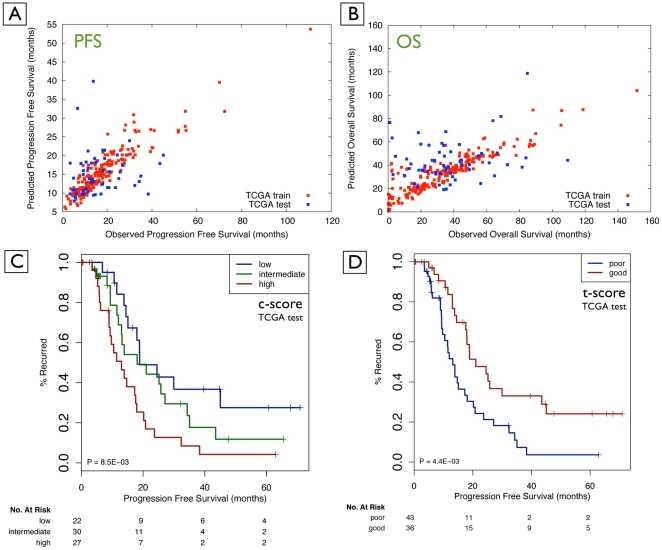
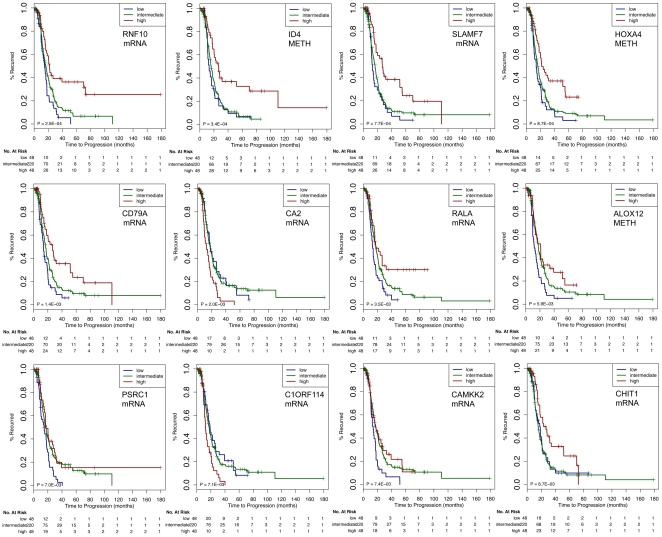
Methodology/principal findings: We implemented a multivariate Cox Lasso model and median time-to-event prediction algorithm and applied it to two datasets integrated from the four genomic data types. We (1) selected features through cross-validation; (2) generated a prognostic index for patient risk stratification; and (3) directly predicted continuous clinical outcome measures, that is, the time to recurrence and survival time. We used Kaplan-Meier p-values, hazard ratios (HR), and concordance probability estimates (CPE) to assess prediction performance, comparing separate and integrated datasets. Data integration resulted in the best PFS signature (withheld data: p-value = 0.008; HR = 2.83; CPE = 0.72).
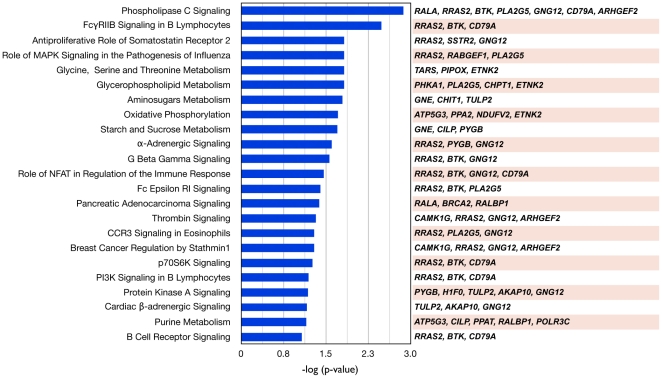
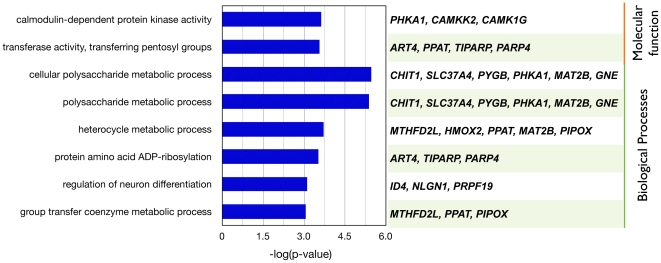
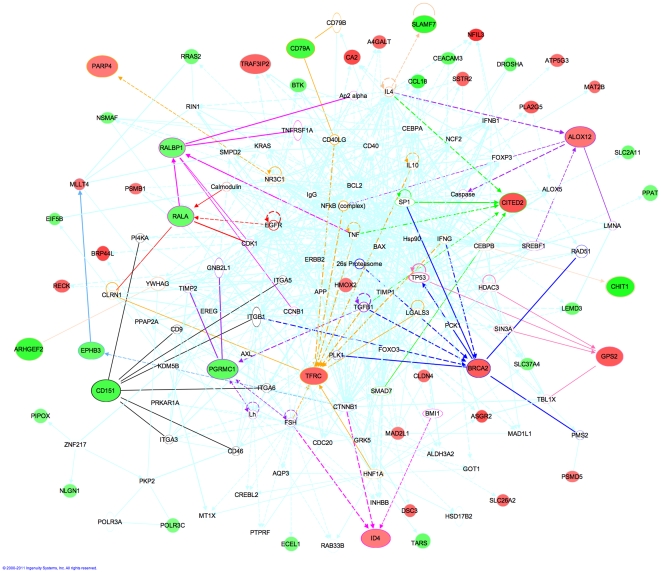
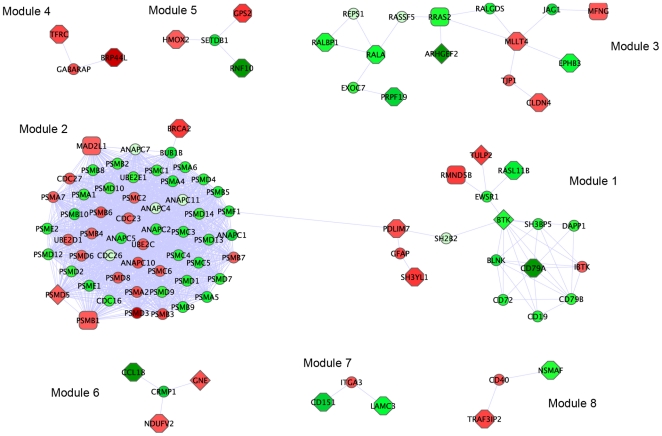
Conclusions/significance: We provide a prediction tool that inputs genomic profiles of primary surgical samples and generates patient-specific predictions for the time to recurrence and survival, along with outcome risk predictions. Using integrated genomic profiles resulted in information gain for prediction of outcomes. Pathway analysis provided potential insights into functional changes affecting disease progression. The prognostic signatures, if prospectively validated, may be useful for interpreting therapeutic outcomes for clinical trials that aim to improve the therapy for SeOvCa patients.
Conflict of interest statement
Figures
References
-
- Dressman HK, Berchuck A, Chan G, Zhai J, Bild A, et al. An integrated genomic-based approach to individualized treatment of patients with advanced-stage ovarian cancer. J Clin Oncol. 2007;25:517–525. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
