

Moderate antiproteinuric effect of add-on aldosterone blockade with eplerenone in non-diabetic chronic kidney disease. A randomized cross-over study
- PMID: 22073219
- PMCID: PMC3208556
- DOI: 10.1371/journal.pone.0026904
Moderate antiproteinuric effect of add-on aldosterone blockade with eplerenone in non-diabetic chronic kidney disease. A randomized cross-over study
Abstract
Background: Reduction of proteinuria and blood pressure (BP) with blockers of the renin-angiotensin system (RAS) impairs the progression of chronic kidney disease (CKD). The aldosterone antagonist spironolactone has an antiproteinuric effect, but its use is limited by side effects. The present study evaluated the short-term antiproteinuric effect and safety of the selective aldosterone antagonist eplerenone in non-diabetic CKD.
Study design: Open randomized cross-over trial.
Setting and participants: Forty patients with non-diabetic CKD and urinary albumin excretion greater than 300 mg/24 hours.
Intervention: Eight weeks of once-daily administration of add-on 25-50 mg eplerenone to stable standard antihypertensive treatment including RAS-blockade.
Outcomes & measurements: 24 hour urinary albumin excretion, BP, p-potassium, and creatinine clearance.
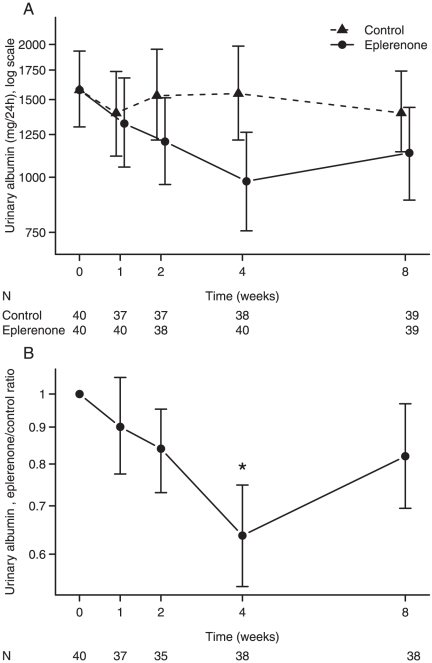
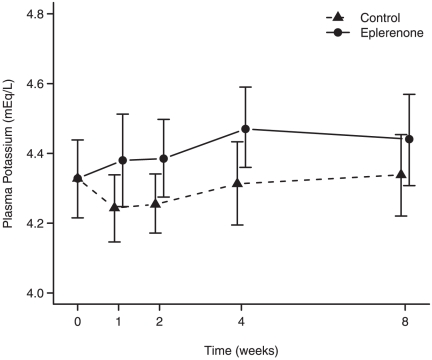
Results: The mean urinary albumin excretion was 22% [CI: 14,28], P < 0.001, lower during treatment with eplerenone. Mean systolic BP was 4 mmHg [CI: 2,6], P = 0.002, diastolic BP was 2 mmHg [CI: 0,4], P = 0.02, creatinine clearance was 5% [CI: 2,8], P = 0.005, lower during eplerenone treatment. After correction for BP and creatinine clearance differences between the study periods, the mean urinary albumin excretion was 14% [CI: 4,24], P = 0.008 lower during treatment. Mean p-potassium was 0.1 mEq/L [CI: 0.1,0.2] higher during eplerenone treatment, P<0.001. Eplerenone was thus well tolerated and no patients were withdrawn due to hyperkalaemia.
Limitations: Open label, no wash-out period and a moderate sample size.
Conclusions: In non-diabetic CKD patients, the addition of eplerenone to standard antihypertensive treatment including RAS-blockade caused a moderate BP independent fall in albuminuria, a minor fall in creatinine clearance and a 0.1 mEq/L increase in p-potassium.
Trial registration: Clinicaltrials.gov NCT00430924.
Conflict of interest statement
Figures
References
-
- de Zeeuw D, Remuzzi G, Parving HH, Keane WF, Zhang Z, et al. Proteinuria, a target for renoprotection in patients with type 2 diabetic nephropathy: lessons from RENAAL. Kidney Int. 2004;65:2309–2320. - PubMed
-
- Jafar TH, Stark PC, Schmid CH, Landa M, Maschio G, et al. Proteinuria as a modifiable risk factor for the progression of non-diabetic renal disease. Kidney Int. 2001;60:1131–1140. - PubMed
-
- Peterson JC, Adler S, Burkart JM, Greene T, Hebert LA, et al. Blood pressure control, proteinuria, and the progression of renal disease. The Modification of Diet in Renal Disease Study. Ann Intern Med. 1995;123:754–762. - PubMed
-
- Ruggenenti P, Perna A, Mosconi L, Pisoni R, Remuzzi G. Urinary protein excretion rate is the best independent predictor of ESRF in non-diabetic proteinuric chronic nephropathies. “Gruppo Italiano di Studi Epidemiologici in Nefrologia” (GISEN). Kidney Int. 1998;53:1209–1216. - PubMed
-
- Ruggenenti P, Perna A, Remuzzi G. Retarding progression of chronic renal disease: the neglected issue of residual proteinuria. Kidney Int. 2003;63:2254–2261. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
