Case Reports
doi: 10.4250/jcu.2011.19.3.152.
Epub 2011 Sep 30.
Left ventricular thrombus associated with takotsubo cardiomyopathy: a cardioembolic cause of cerebral infarction
Affiliations
- PMID: 22073327
- PMCID: PMC3209596
- DOI: 10.4250/jcu.2011.19.3.152
Item in Clipboard
Case Reports
Left ventricular thrombus associated with takotsubo cardiomyopathy: a cardioembolic cause of cerebral infarction
J Cardiovasc Ultrasound.
2011 Sep.
Abstract
Takotsubo cardiomyopathy, also called stress-induced cardiomyopathy, usually occurs in patients with severe emotional or physiologic stress. The prognosis is favorable, and the wall motion abnormlities normalize within weeks. However, stress-induced cardiomyopathy is rarely assosicated with left ventricular thrombus and thromboembolic complications. Here, we report a case of stress-induced cardiomyopathy with left ventricular thrombus that embolized to cause cerebral infarction.
Keywords: Cerebral infarction; Takotsubo cardiomyopathy; Thrombus.
Figures
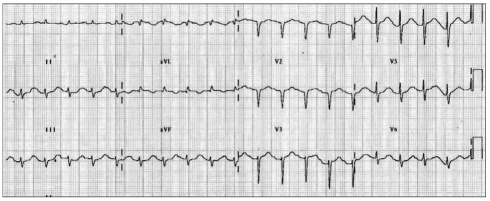
An electrocardiogram showing an abnormal Q wave in the anterior precordial leads and a prolonged QT interval.
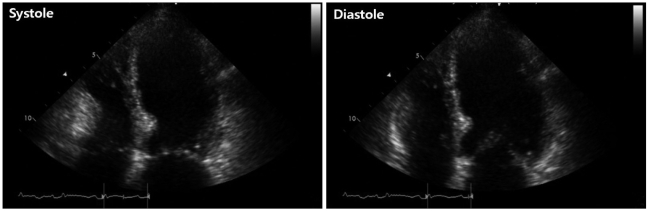
Initial transthoracic echocardiographic image in the apical 4-chamber view showing left ventricular apical ballooning and dyskinesis.
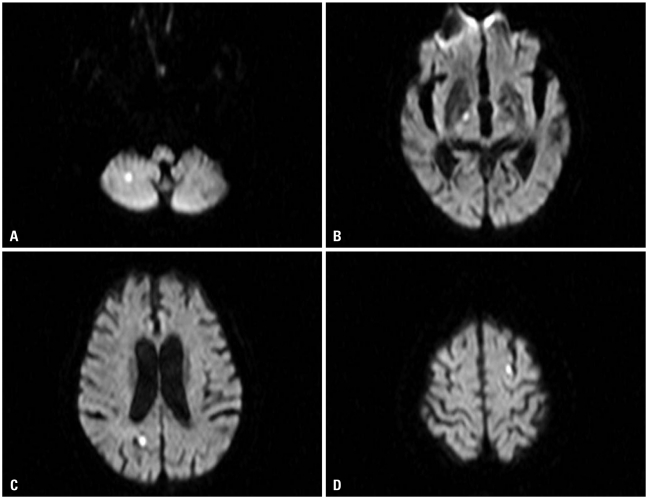
Diffusion image of magnetic resonance imaging showed multiple diffusion restrictive lesions in right cerebellar hemisphere (A), right internal capsule (B), right occipital lobe (C), and left parietal lobe (D).
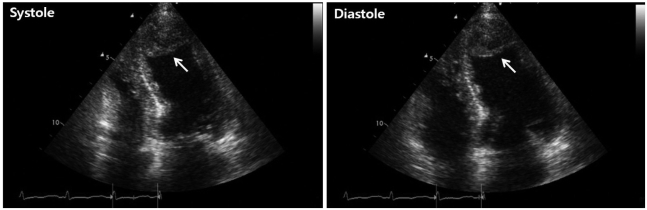
Transthoracic echocardiographic image obtained after cerebral infarction developed, shows a 24 × 25 mm thrombus (arrow) in the left ventricular apex.
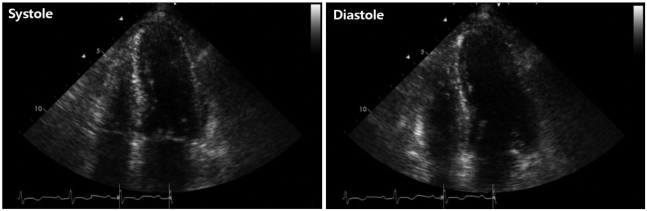
Transthoracic echocardiographic image obtained after 1 week of anticoagulation therapy shows near normal left ventricular wall motion and complete resolution of the apical thrombus.
References
-
- Wittstein IS, Thiemann DR, Lima JA, Baughman KL, Schulman SP, Gerstenblith G, Wu KC, Rade JJ, Bivalacqua TJ, Champion HC. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med. 2005;352:539–548. - PubMed
-
- Prasad A. Apical ballooning syndrome: an important differential diagnosis of acute myocardial infarction. Circulation. 2007;115:e56–e59. - PubMed
-
- Akashi YJ, Tejima T, Sakurada H, Matsuda H, Suzuki K, Kawasaki K, Tsuchiya K, Hashimoto N, Musha H, Sakakibara M, Nakazawa K, Miyake F. Left ventricular rupture associated with Takotsubo cardiomyopathy. Mayo Clin Proc. 2004;79:821–824. - PubMed
-
- Kim DH, Bang DW, Ahn JH, Park SH, Oh HS, Yoon YJ, Hyon MS, Kim SK, Kwon YJ. Three cases of stress induced transient LV dysfunction: stress induced cardiomyopathy. J Korean Soc Echocardiogr. 2005;13:83–86.
Publication types
LinkOut - more resources
Full Text Sources