

Laparoscopic low anterior resection for hematogenous rectal metastasis from gastric adenocarcinoma: a case report
- PMID: 22074191
- PMCID: PMC3230135
- DOI: 10.1186/1477-7819-9-148
Laparoscopic low anterior resection for hematogenous rectal metastasis from gastric adenocarcinoma: a case report
Abstract
Background: Gastric cancer is one of the most common malignancies in the world and is the second most common cause of cancer-related death in Korea. Colorectal metastases from gastric adenocarcinoma are known to be very rare. We report an unusual case of rectal metastasis of gastric adenocarcinoma.
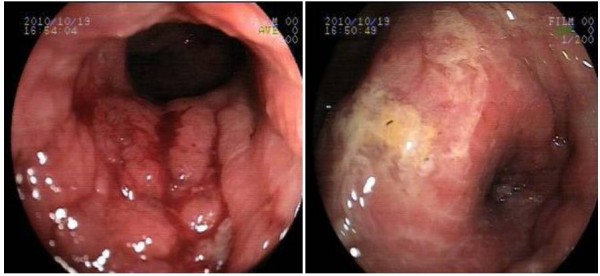
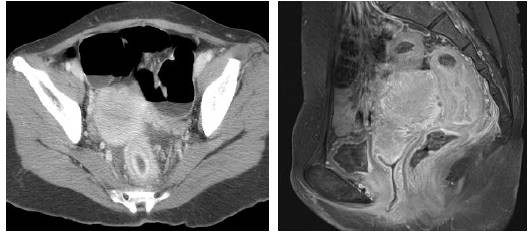
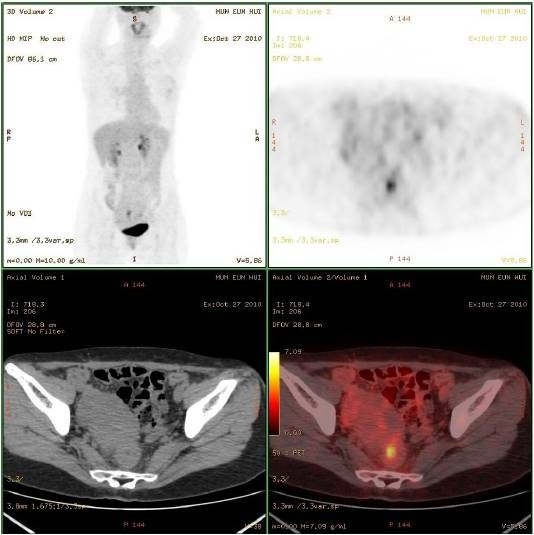
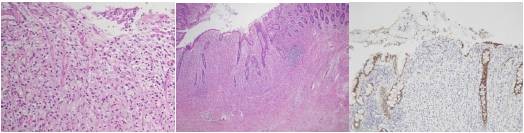
Case presentation: We report a case of a 43-year-old female patient with gastric cancer who first presented with epigastric pain. The endoscopic and radiologic findings were suggestive of Borrmann type III advanced gastric cancer with linitis plastica. Radical total gastrectomy with D2 lymph node dissection was performed. The pathology report was AJCC TNM Stage II gastric adenocarcinoma (T3N0M0). On follow up at 34 months after surgery, the patient complained of difficulty in defecation. On colonoscopy, a hard, indurated extraluminal mass was detected 7 cm proximal to the anal verge. The biopsy demonstrated chronic nonspecific colitis. Abdominal CT, rectal MRI and PET-CT revealed rectal metastasis from gastric cancer. Laparoscopic ultralow anterior resection with diverting ileostomy was performed. The pathology report was metastatic adenocarcinoma, and this diagnosis was identical to the gastric pathology reported in the previous pathology report. The patient was discharged after the 11th postoperative day with no adverse events.
Conclusion: Rectal metastasis from gastric cancer is known to be very rare. However, metastatic gastric adenocarcinoma should be considered as a differential diagnosis for patients presenting with a colorectal mass and a past history of gastric cancer.
Figures

References
-
- Niinobu T, Nakagawa S, Itani Y, Nishikawa Y, Amano M, Higaki N, Hayashida H, Sakon M. [Rectal stenosis due to Schnitzler metastasis following surgery for gastric cancer--a case successfully treated with TS-1 and CDDP combination chemotherapy] Gan To Kagaku Ryoho. 2005;32:1761–1764. - PubMed
-
- Green FLPD, Fleming ID, Fritz A, Balch CM, Haller DG, (Ed) American Joint Committee on Cancer (2002) AJCC cancer staging manual. 6. New York: Springer; 2002.
-
- Marrelli D, Roviello F, de Manzoni G, Morgagni P, Di Leo A, Saragoni L, De Stefano A, Folli S, Cordiano C, Pinto E. Different patterns of recurrence in gastric cancer depending on Lauren's histological type: longitudinal study. World J Surg. 2002;26:1160–1165. doi: 10.1007/s00268-002-6344-2. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
