

The influence of induction therapy for kidney transplantation after a non-renal transplant
- PMID: 22076872
- PMCID: PMC3265339
- DOI: 10.2215/CJN.02360311
The influence of induction therapy for kidney transplantation after a non-renal transplant
Abstract
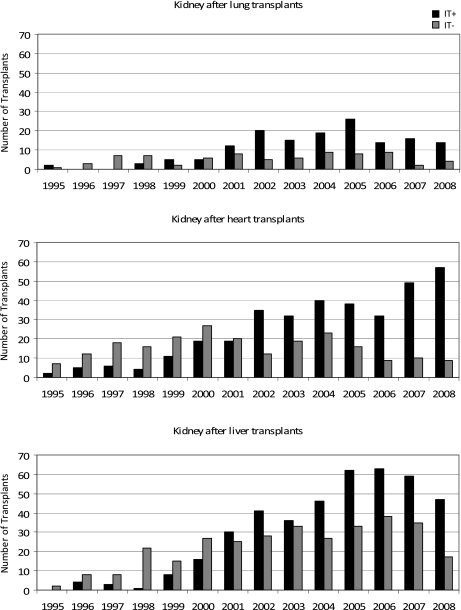
Background and objectives: Non-renal transplant recipients who subsequently develop ESRD and undergo kidney transplantation are medically and immunologically complex due to comorbidities, high cumulative exposure to immunosuppressants, and sensitization to alloantigen from the prior transplant. Although prior non-renal transplant recipients are one of the fastest growing segments of the kidney wait list, minimal data exist to guide the use of antibody induction therapy (IT+) at the time of kidney after lung (KALu), heart (KAH), and liver (KALi) transplant.
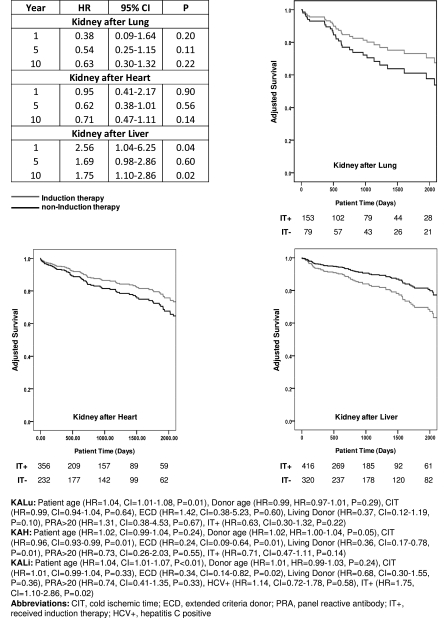
Design, setting, participants, & measurements: This retrospective cohort study used national registry data to examine IT use and survival after kidney transplantation. Separate multivariate Cox regression models were constructed to assess patient survival for IT+ and IT- KALu (n=232), KAH (n=588), and KALi (n=736) recipients.
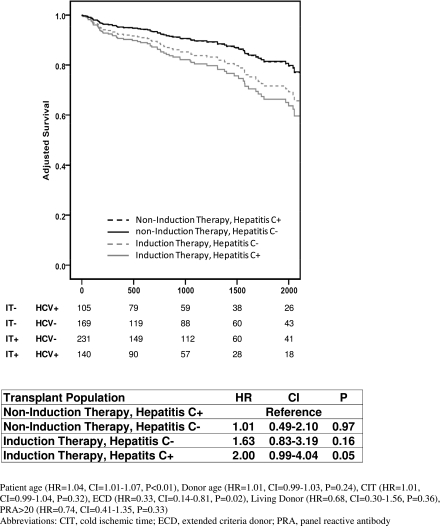
Results: Use of IT increased during the study period. The percentage of patients considered highly sensitized (panel reactive antibody ≥20%) was not statistically significant between IT+ and IT- groups. IT+ was not associated with improvement in 1- and 10-year patient survival for KALu (P=0.20 and P=0.22, respectively) or for KAH (P=0.90 and P=0.14, respectively). However, IT+ among KALi was associated with inferior patient survival at 1 and 10 years (P=0.04 and P=0.02, respectively).
Conclusions: Use of IT for kidney transplantation among prior non-renal transplant recipients may not offer a survival advantage in KALu or KAH. However, due to limited power, these findings should be interpreted cautiously. IT+ was associated with inferior outcomes for KALi. Use of IT should be judicially reconsidered in this complex group of recipients.
Figures
References
-
- Chandrakantan A, de Mattos AM, Naftel D, Crosswy A, Kirklin J, Curtis JJ: Increasing referral for renal transplant evaluation in recipients of nonrenal solid-organ transplants: A single-center experience. Clin J Am Soc Nephrol 1: 832–836, 2006 - PubMed
-
- Bennett WM, DeMattos A, Meyer MM, Andoh T, Barry JM: Chronic cyclosporine nephropathy: The Achilles’ heel of immunosuppressive therapy. Kidney Int 50: 1089–1100, 1996 - PubMed
-
- Lindelöw B, Bergh CH, Herlitz H, Waagstein F: Predictors and evolution of renal function during 9 years following heart transplantation. J Am Soc Nephrol 11: 951–957, 2000 - PubMed
-
- Hamour IM, Omar F, Lyster HS, Palmer A, Banner NR: Chronic kidney disease after heart transplantation. Nephrol Dial Transplant 24: 1655–1662, 2009 - PubMed
-
- Ojo AO, Held PJ, Port FK, Wolfe RA, Leichtman AB, Young EW, Arndorfer J, Christensen L, Merion RM: Chronic renal failure after transplantation of a nonrenal organ. N Engl J Med 349: 931–940, 2003 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
