

Vascular access sites for acute renal replacement in intensive care units
- PMID: 22076877
- PMCID: PMC3265351
- DOI: 10.2215/CJN.06570711
Vascular access sites for acute renal replacement in intensive care units
Abstract
Background and objectives: Several temporary venous catheterizations are sometimes required for acute renal replacement therapy (RRT) in the intensive care unit (ICU). This study compares first and second catheterizations in the femoral and jugular veins in terms of patient safety.
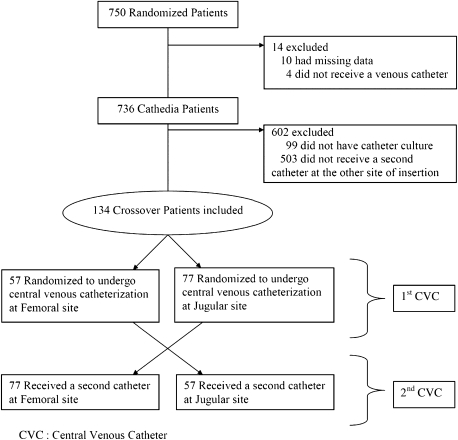
Design, setting, participants, & measurements: A crossover study from the catheter-dialysis randomized study (Cathedia), which was conducted among 736 critically ill adults requiring RRT, was performed. Catheter insertion complications, catheter-tip colonization, catheter dysfunction and urea reduction ratio (URR) were analyzed considering the crossover and longitudinal designs.
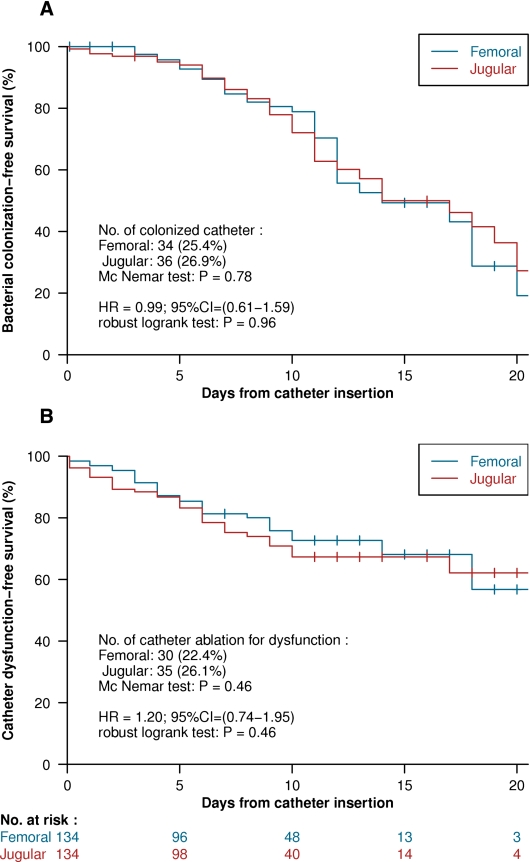
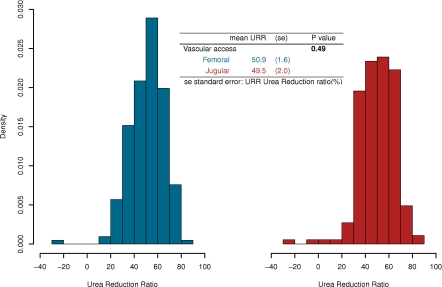
Results: This study analyzed 134 patients who underwent two different sites of catheterization, 57 and 77 of whom were initially randomized in the femoral and jugular site, respectively. Using anatomic landmarks, time to insert a femoral catheter was shorter (P=0.01) and more successful (P=0.003) compared with catheterization in the jugular site. Time to catheter-tip colonization at removal was not significantly different between the two sites of insertion (median, 14 days in both groups; hazard ratio, 0.99; 95% confidence interval, 0.61-1.59; P=0.96), as well as time to dysfunction. URRs were analyzed from 395 dialysis sessions (n=48 patients). No significant difference (P=0.49) in mean URR was detected between sessions performed through femoral (n=213; 50.9%) and jugular (n=182; 49.5%) dialysis catheters.
Conclusions: These results validate prior results of this study group and extend external validity to the second catheter used for RRT in the ICU. Femoral and internal jugular acute vascular access sites are both acceptable for RRT therapy in the ICU.
Figures
References
-
- Schetz M: Vascular access for HD and CRRT. Contrib Nephrol 156: 275–286, 2007 - PubMed
-
- Mermel LA: Prevention of intravascular catheter-related infections. Ann Intern Med 132: 391–402, 2000 - PubMed
-
- McGee DC, Gould MK: Preventing complications of central venous catheterization. N Engl J Med 348: 1123–1133, 2003 - PubMed
-
- Oliver MJ, Callery SM, Thorpe KE, Schwab SJ, Churchill DN: Risk of bacteremia from temporary hemodialysis catheters by site of insertion and duration of use: A prospective study. Kidney Int 58: 2543–2545, 2000 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
