

Predictors of sudden cardiac death: a competing risk approach in the hemodialysis study
- PMID: 22076880
- PMCID: PMC3265355
- DOI: 10.2215/CJN.06320611
Predictors of sudden cardiac death: a competing risk approach in the hemodialysis study
Abstract
Background and objectives: There are few data on risk factors for sudden cardiac death (SCD) in patients undergoing hemodialysis (HD). The study objective was to identify predictors associated with various causes of death in the Hemodialysis (HEMO) Study and to develop a prediction model for SCD using a competing risk approach.
Design, setting, participants, & measurements: In this analysis of 1745 HEMO participants, all-cause mortality was classified as SCD, non-SCD, and noncardiac death. Predictors for each cause of death were evaluated using cause-specific Cox proportional hazards models, and a competing risk approach was used to calculate absolute risk predictions for SCD.
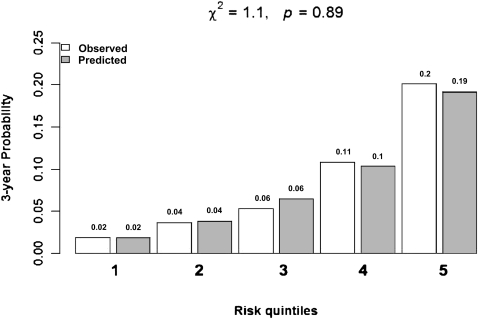
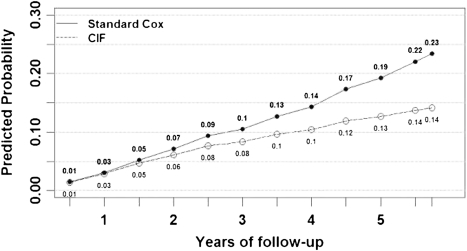
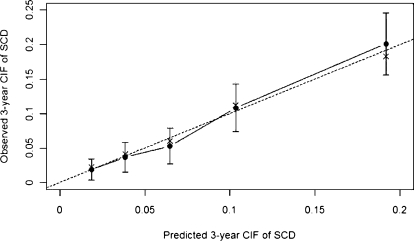
Results: During a median follow-up of 2.5 years, 808 patients died. Rates of SCD, non-SCD, and noncardiac death were 22%, 17%, and 61%, respectively. Predictors of various causes of death differ somewhat in HD patients. Age, diabetes, peripheral vascular disease, ischemic heart disease, serum creatinine, and alkaline phosphatase were independent predictors of SCD. The 3-year C-statistic for SCD was 0.75 (95% confidence interval, 0.70-0.79), and calibration was good (χ(2)=1.1; P=0.89). At years 3 and 5 of follow-up, the standard Cox model overestimated the risk for SCD as compared with the competing risk approach on the relative scale by 25% and 46%, respectively, and on the absolute scale by 2% and 6%, respectively.
Conclusions: Predictors of various causes of death differ in HD patients. The proposed prediction model for SCD accounts for competing causes of death. External validation of this model is required.
Figures
Comment in
-
Expect the unexpected: sudden cardiac death in dialysis patients.Clin J Am Soc Nephrol. 2012 Jan;7(1):8-11. doi: 10.2215/CJN.12131111. Epub 2011 Dec 15. Clin J Am Soc Nephrol. 2012. PMID: 22173859 No abstract available.
References
-
- U.S. Renal Data System: USRDS 2008 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2008
-
- Bleyer AJ, Hartman J, Brannon PC, Reeves-Daniel A, Satko SG, Russell G: Characteristics of sudden death in hemodialysis patients. Kidney Int 69: 2268–2273, 2006 - PubMed
-
- Bleyer AJ, Russell GB, Satko SG: Sudden and cardiac death rates in hemodialysis patients. Kidney Int 55: 1553–1559, 1999 - PubMed
-
- Ganesh SK, Stack AG, Levin NW, Hulbert-Shearon T, Port FK: Association of elevated serum PO(4), Ca x PO(4) product, and parathyroid hormone with cardiac mortality risk in chronic hemodialysis patients. J Am Soc Nephrol 12: 2131–2138, 2001 - PubMed
-
- Green D, Roberts PR, New DI, Kalra PA: Sudden cardiac death in hemodialysis patients: an in-depth review. Am J Kidney Dis 57: 921–929, 2011 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
