

Transition zones between healthy and diseased retina in choroideremia (CHM) and Stargardt disease (STGD) as compared to retinitis pigmentosa (RP)
- PMID: 22076985
- PMCID: PMC3341121
- DOI: 10.1167/iovs.11-8554
Transition zones between healthy and diseased retina in choroideremia (CHM) and Stargardt disease (STGD) as compared to retinitis pigmentosa (RP)
Abstract
Purpose: To describe the structural changes across the transition zone (TZ) in choroideremia (CHM) and Stargardt disease (STGD) and to compare these to the TZ in retinitis pigmentosa (RP).
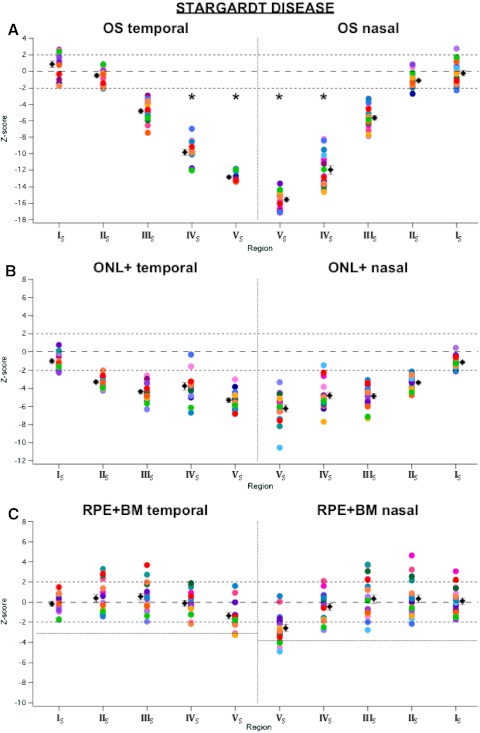
Methods: Frequency-domain (Fd)OCT line scans were obtained from seven patients with CHM, 20 with STGD, and 12 with RP and compared with those of 30 previously studied controls. A computer-aided manual segmentation procedure was used to determine the thicknesses of the outer segment (OS) layer, the outer nuclear layer plus outer plexiform layer (ONL+), the retinal pigment epithelium plus Bruch's membrane (RPE+BM), and the outer retina (OR).
Results: The TZ, while consistent within patient groups, showed differences across disease groups. In particular, (1) OS loss occurred before ONL+ loss in CHM and RP, whereas ONL+ loss occurred before OS loss in STGD; (2) ONL+ was preserved over a wider region of the retina in CHM than in RP; (3) RPE+BM remained normal across the RP TZ, but was typically thinned in CHM. In some CHM patients, it was abnormally thin in regions with normal OS and ONL+ thickness. In STGD, RPE+BM was thinned by the end of the TZ; and (4) the disappearances of the IS/OS and OLM were more abrupt in CHM and STGD than in RP.
Conclusions: On fdOCT scans, patients with RP, CHM, and STGD all have a TZ between relatively healthy and severely affected retina. The patterns of changes in the receptor layers are similar within a disease category, but different across categories. The findings suggest that the pattern of progression of each disease is distinct and may offer clues for strategies in the development of future therapies.
Figures






References
-
- Jacobson SG, Aleman TS, Sumaroka A, et al. Disease boundaries in the retina of patients with Usher syndrome caused by MYO7A gene mutations. Invest Ophthalmol Vis Sci. 2009;50:1886–1894 - PubMed
-
- Jacobson SG, Cideciyan AV, Sumaroka A, et al. Remodeling of the human retina in choroideremia: Rab escort protein 1 (REP-1) mutations. Invest Ophthalmol Vis Sci. 2006;47:4113–4120 - PubMed
-
- Lee TK, McTaggart KE, Sleving PA, et al. Clinical diagnoses that overlap with choroideremia. Can J Ophthalmol. 2003;38:364–372 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
