

Intensive diabetes therapy and glomerular filtration rate in type 1 diabetes
- PMID: 22077236
- PMCID: PMC3270008
- DOI: 10.1056/NEJMoa1111732
Intensive diabetes therapy and glomerular filtration rate in type 1 diabetes
Abstract
Background: An impaired glomerular filtration rate (GFR) leads to end-stage renal disease and increases the risks of cardiovascular disease and death. Persons with type 1 diabetes are at high risk for kidney disease, but there are no interventions that have been proved to prevent impairment of the GFR in this population.
Methods: In the Diabetes Control and Complications Trial (DCCT), 1441 persons with type 1 diabetes were randomly assigned to 6.5 years of intensive diabetes therapy aimed at achieving near-normal glucose concentrations or to conventional diabetes therapy aimed at preventing hyperglycemic symptoms. Subsequently, 1375 participants were followed in the observational Epidemiology of Diabetes Interventions and Complications (EDIC) study. Serum creatinine levels were measured annually throughout the course of the two studies. The GFR was estimated with the use of the Chronic Kidney Disease Epidemiology Collaboration formula. We analyzed data from the two studies to determine the long-term effects of intensive diabetes therapy on the risk of impairment of the GFR, which was defined as an incident estimated GFR of less than 60 ml per minute per 1.73 m(2) of body-surface area at two consecutive study visits.
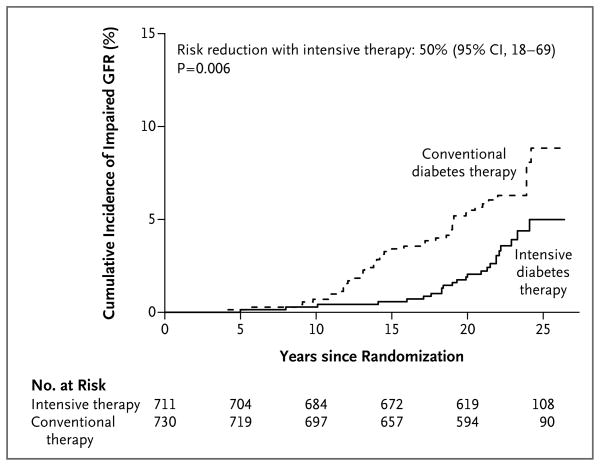
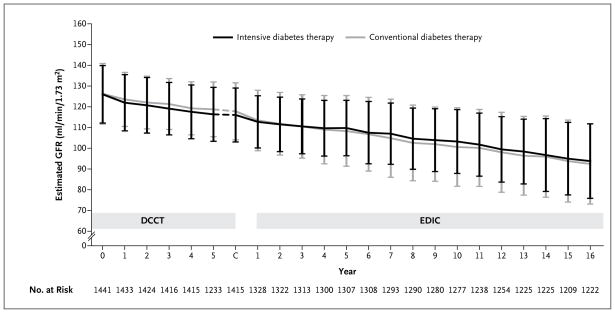
Results: Over a median follow-up period of 22 years in the combined studies, impairment of the GFR developed in 24 participants assigned to intensive therapy and in 46 assigned to conventional therapy (risk reduction with intensive therapy, 50%; 95% confidence interval, 18 to 69; P=0.006). Among these participants, end-stage renal disease developed in 8 participants in the intensive-therapy group and in 16 in the conventional-therapy group. As compared with conventional therapy, intensive therapy was associated with a reduction in the mean estimated GFR of 1.7 ml per minute per 1.73 m(2) during the DCCT study but during the EDIC study was associated with a slower rate of reduction in the GFR and an increase in the mean estimated GFR of 2.5 ml per minute per 1.73 m(2) (P<0.001 for both comparisons). The beneficial effect of intensive therapy on the risk of an impaired GFR was fully attenuated after adjustment for glycated hemoglobin levels or albumin excretion rates.
Conclusions: The long-term risk of an impaired GFR was significantly lower among persons treated early in the course of type 1 diabetes with intensive diabetes therapy than among those treated with conventional diabetes therapy. (Funded by the National Institute of Diabetes and Digestive and Kidney Diseases and others; DCCT/EDIC ClinicalTrials.gov numbers, NCT00360815 and NCT00360893.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Diabetes: Intensive glucose control in type 1 diabetes mellitus reduces risk of GFR loss.Nat Rev Endocrinol. 2011 Dec 6;8(2):65. doi: 10.1038/nrendo.2011.214. Nat Rev Endocrinol. 2011. PMID: 22143184 No abstract available.
-
Diabetes: Intensive glucose control in type 1 diabetes mellitus reduces risk of GFR loss.Nat Rev Nephrol. 2011 Dec 6;8(1):1. doi: 10.1038/nrneph.2011.176. Nat Rev Nephrol. 2011. PMID: 22143332 No abstract available.
-
Intensive therapy and GFR in type 1 diabetes.N Engl J Med. 2012 Mar 1;366(9):856; author reply 857-8. doi: 10.1056/NEJMc1200746. N Engl J Med. 2012. PMID: 22375980 No abstract available.
-
Intensive therapy and GFR in type 1 diabetes.N Engl J Med. 2012 Mar 1;366(9):856-7; author reply 857-8. doi: 10.1056/NEJMc1200746. N Engl J Med. 2012. PMID: 22375981 No abstract available.
-
Intensive therapy and GFR in type 1 diabetes.N Engl J Med. 2012 Mar 1;366(9):857; author reply 857-8. doi: 10.1056/NEJMc1200746. N Engl J Med. 2012. PMID: 22375982 No abstract available.
-
Diabetes: treating diabetic nephropathy-still an unresolved issue.Nat Rev Endocrinol. 2012 Sep;8(9):515-6. doi: 10.1038/nrendo.2012.125. Epub 2012 Jul 24. Nat Rev Endocrinol. 2012. PMID: 22825399 No abstract available.
-
[Improvement of glomerular filtration rate by intensified insulin therapy : the DCCT and EDIC studies].Internist (Berl). 2012 Nov;53(11):1376-8. doi: 10.1007/s00108-012-3161-z. Internist (Berl). 2012. PMID: 23069781 German. No abstract available.
References
-
- Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting–enzyme inhibition on diabetic nephropathy. N Engl J Med. 1993;329:1456–62. [Erratum, N Engl J Med 1993;330:152.] - PubMed
-
- Lewis EJ, Hunsicker LG, Clarke WR, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851–60. - PubMed
-
- Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001;345:861–9. - PubMed
-
- The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–86. - PubMed
-
- Effect of intensive therapy on the development and progression of diabetic nephropathy in the Diabetes Control and Complications Trial. Kidney Int. 1995;47:1703–20. Idem. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical