

Microthrombosis after experimental subarachnoid hemorrhage: time course and effect of red blood cell-bound thrombin-activated pro-urokinase and clazosentan
- PMID: 22079156
- PMCID: PMC5505050
- DOI: 10.1016/j.expneurol.2011.10.029
Microthrombosis after experimental subarachnoid hemorrhage: time course and effect of red blood cell-bound thrombin-activated pro-urokinase and clazosentan
Abstract
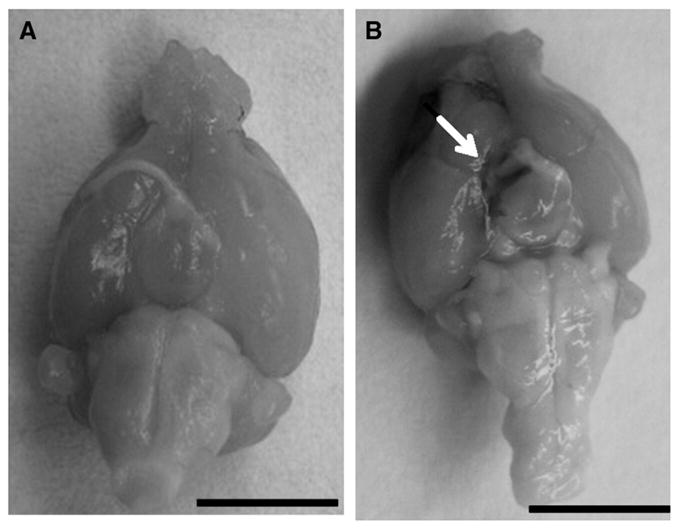
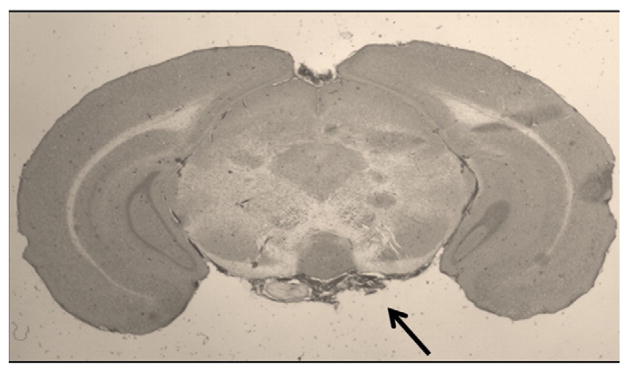
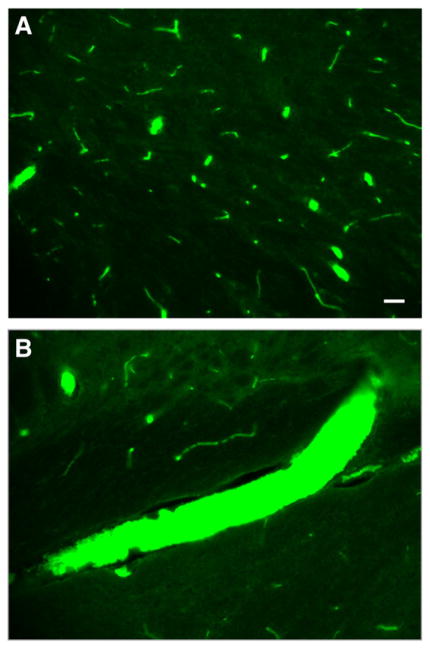
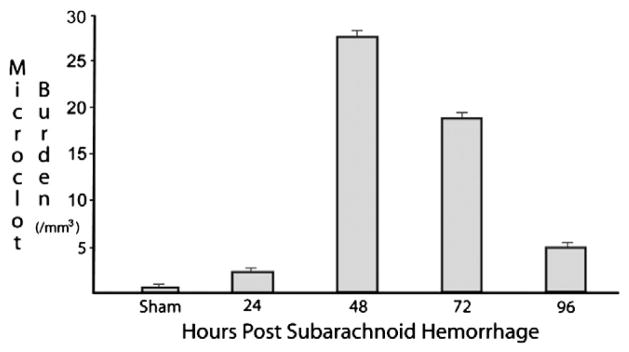
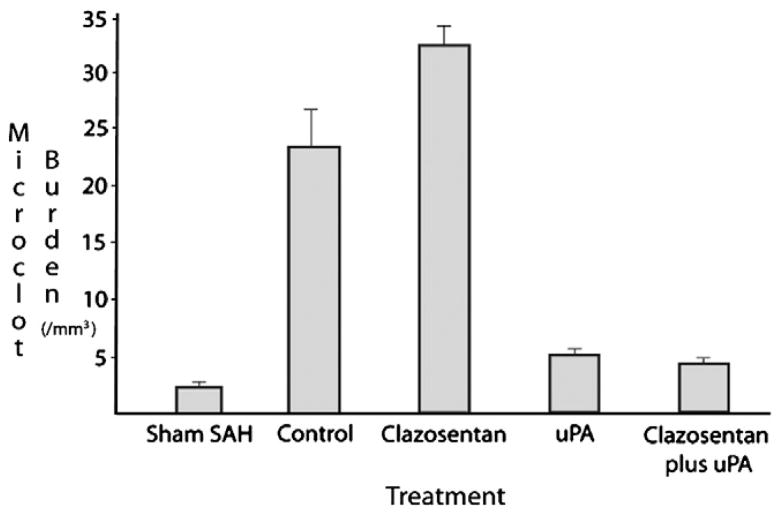
Delayed cerebral ischemia (DCI) is a significant cause of morbidity and mortality for patients surviving the rupture of an intracranial aneurysm. Despite an association between vasospasm and DCI, thrombosis and thromboembolism may also contribute to DCI. In this study we investigate the time course of intravascular microclot formation after experimental subarachnoid hemorrhage (SAH) and assess the effects of the following two drugs on microclot burden: mutant thrombin-activated urokinase-type plasminogen activator (scFv/uPA-T), which is bound to red blood cells for use as a thromboprophylactic agent, and clazosentan, an endothelin antagonist. In the first study, adult male C57BL/6 mice were sacrificed at 24 (n=5), 48 (n=6), 72 (n=8), and 96 (n=3) hours after SAH induced by filament perforation of the anterior cerebral artery. Sham animals (n=5) underwent filament insertion without puncture. In the second study, animals received scFv/uPA-T (n=5) 3 hours after hemorrhage, clazosentan (n=5) by bolus and subcutaneous pump after SAH just prior to skin closure, or a combination of scFv/uPA-T and clazosentan (n=4). Control (n=6) and sham (n=5) animals received saline alone. All animals were sacrificed at 48 hours and underwent intra-cardiac perfusion with 4% paraformaldehyde. The brains were then extracted and sliced coronally on a cryostat and processed for immunohistochemistry. An antibody recognizing thrombin-anti-thrombin complexes was used to detect microclots on coronal slices. Microclot burden was calculated for each animal and compared among groups. Following SAH, positive anti-thrombin staining was detected bilaterally in the following brain regions, in order of decreasing frequency: cortex; hippocampus; hypothalamus; basal ganglia. Few microclots were found in the shams. Microclot burden peaked at 48 hours and then decreased gradually. Animals receiving scFv/uPA-T and scFv/uPA-T+clazosentan had a lower microclot burden than controls, whereas animals receiving clazosentan alone had a higher microclot burden (p<0.005). The overall mortality rate in the time course study was 40%; mortality was highest among control animals in the second study. Intravascular microclots form in a delayed fashion after experimental SAH. Microclots may be safely reduced using a novel form of thromboprophylaxis provided by RBC-targeted scFv/uPA-T and represent a potential target for therapeutic intervention in the treatment of DCI.
Copyright © 2011. Published by Elsevier Inc.
Figures
References
-
- Allen GS, Ahn HS, Preziosi TJ, Battye R, Boone SC, Boone SC, Chou SN, Kelly DL, Weir BK, Crabbe RA, Lavik PJ, Rosenbloom SB, Dorsey FC, Ingram CR, Mellits DE, Bertsch LA, Boisvert DP, Hundley MB, Johnson RK, Strom JA, Transou CR. Cerebral arterial spasm—a controlled trial of nimodipine in patients with sub-arachnoid hemorrhage. N Engl J Med. 1983;308:619–624. - PubMed
-
- Amin-Hanjani S, Ogilvy CS, Barker FG., II Does intracisternal thrombolysis prevent vasospasm after aneurysmal subarachnoid hemorrhage? A meta-analysis Neurosurgery. 2004;54:326–334. discussion 334–5. - PubMed
-
- Antovic J, Bakic M, Zivkovic M, Ilic A, Blomback M. Blood coagulation and fibrinolysis in acute ischaemic and haemorrhagic (intracerebral and subarachnoid haemorrhage) stroke: does decreased plasmin inhibitor indicate increased fibrinolysis in subarachnoid haemorrhage compared to other types of stroke? Scand J Clin Lab Invest. 2002;62:195–199. - PubMed
-
- Collen D, Lu HR, Lijnen HR, Nelles L, Stassen JM. Thrombolytic and pharmacokinetic properties of chimeric tissue-type and urokinase-type plasminogen activators. Circulation. 1991;84:1216–1234. - PubMed
-
- Crompton MR. The pathogenesis of cerebral infarction following the rupture of cerebral berry aneurysms. Brain. 1964;87:491–510. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
