

Immunologic criteria are poor predictors of virologic outcome: implications for HIV treatment monitoring in resource-limited settings
- PMID: 22080121
- PMCID: PMC3246873
- DOI: 10.1093/cid/cir729
Immunologic criteria are poor predictors of virologic outcome: implications for HIV treatment monitoring in resource-limited settings
Abstract
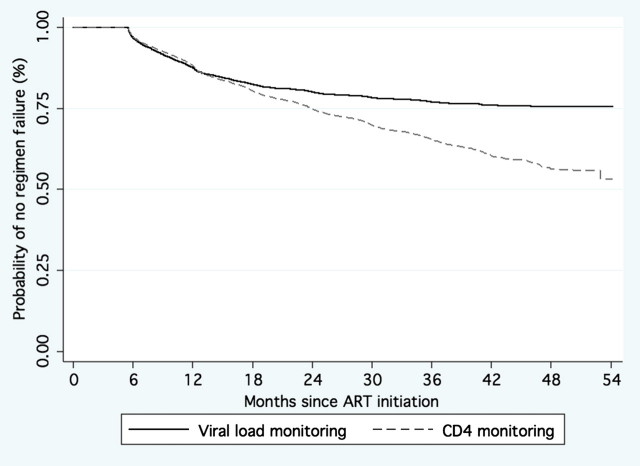
Background: Viral load (VL) quantification is considered essential for determining antiretroviral treatment (ART) success in resource-rich countries. However, it is not widely available in resource-limited settings where the burden of human immunodeficiency virus infection is greatest. In the absence of VL monitoring, switches to second-line ART are based on World Health Organization (WHO) clinical or immunologic failure criteria.
Methods: We assessed the performance of CD4 cell criteria to predict virologic outcomes in a large ART program in Nigeria. Laboratory monitoring consists of CD4 cell count and VL at baseline, then every 6 months. Failure was defined as 2 consecutive VLs >1000 copies/mL after at least 6 months of ART. Virologic outcomes were compared with the 3 WHO-defined immunologic failure criteria.
Results: A total of 9690 patients were included in the analysis (median follow-up, 33.2 months). A total of 1225 patients experienced failure by both immunologic and virologic criteria, 872 by virologic criteria only, and 1897 by immunologic criteria only. The sensitivity of CD4 cell criteria to detect viral failure was 58%, specificity was 75%, and the positive-predictive value was 39%. For patients with both virologic and immunologic failure, VL criteria identified failure significantly earlier than CD4 cell criteria (median, 10.4 vs 15.6 months; P < .0001).
Conclusions: Because of the low sensitivity of immunologic criteria, a substantial number of failures are missed, potentially resulting in accumulation of resistance mutations. In addition, specificity and predictive values are low, which may result in large numbers of unnecessary ART switches. Monitoring solely by immunologic criteria may result in increased costs because of excess switches to more expensive ART and development of drug-resistant virus.
Figures
References
-
- WHO/UNAIDS/UNICEF. Towards universal access: Scaling up priority HIV/AIDS interventions in the health sector. Progress report 2010. Geneva, Switzerland: WHO Press; 2010.
-
- Thompson MA, Aberg JA, Cahn P, et al. Antiretroviral treatment of adult HIV infection: 2010 recommendations of the International AIDS Society-USA Panel. JAMA. 2010;304:321–33. - PubMed
-
- Clumeck N, Monforte A, Gatell J, Battegay M, et al. The EACS Executive Committee. Clinical management and treatment of HIV infected adults in Europe. EACS guidelines. 2011. Version 5–4. www.europeanaidsclinicalsociety.org/. Accessed 18 July 2011. - PubMed
-
- Hornberger J, Holodniy M, Robertus K, et al. A systematic review of cost-utility analyses in HIV/AIDS: implications for public policy. Med Decis Making. 2007;27:789–821. - PubMed
-
- Mellors JW, Muñoz A, Giorgi JV, et al. Plasma viral load and CD4+ lymphocytes as prognostic markers of HIV-1 infection. Ann Intern Med. 1997;126:946–54. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
