

Clinical outcomes of type III Pseudomonas aeruginosa bacteremia
- PMID: 22080633
- PMCID: PMC3288436
- DOI: 10.1097/CCM.0b013e3182377906
Clinical outcomes of type III Pseudomonas aeruginosa bacteremia
Abstract
Background: Pseudomonas aeruginosa bacteremia is a serious and life-threatening infection associated with high mortality. Among the multitude of virulence determinants possessed by P. aeruginosa, the type 3 secretion system has been implicated with more acute and invasive infection in respiratory diseases. However, the relationship between the type 3 secretion system and clinical outcomes in P. aeruginosa bacteremia has not been investigated.
Objectives: To determine the association between the type 3 secretion system virulence factor in P. aeruginosa bloodstream infection and 30-day mortality.
Design: Retrospective analysis of 85 cases of P. aeruginosa bacteremia.
Setting: Tertiary care hospital.
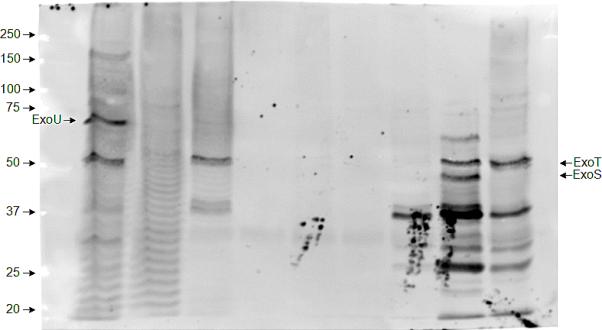
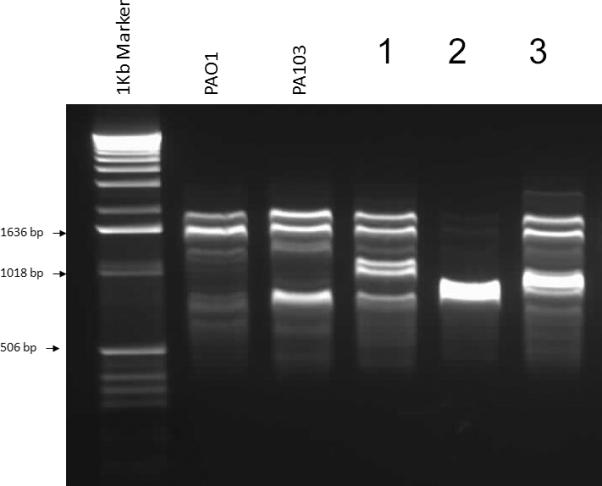
Interventions: Bacterial isolates were assayed in vitro for secretion of type 3 exotoxins (ExoU, ExoT, and ExoS). Strain relatedness was analyzed using randomly amplified polymorphic DNA polymerase chain reaction genotyping. Antimicrobial susceptibilities were determined by means of the Kirby-Bauer disk-diffusion test.
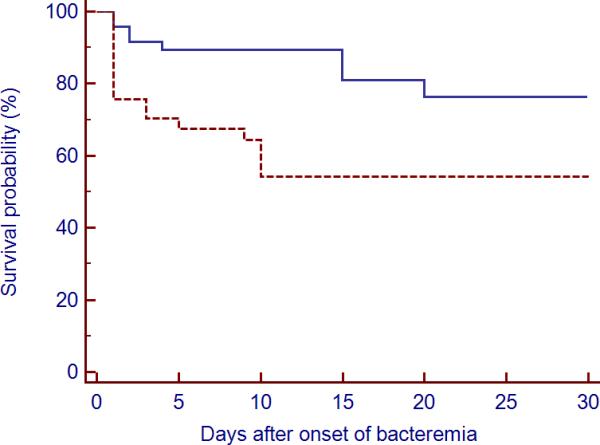
Measurements and main results: At least one of the type 3 secretion system proteins was detected in 37 out of the 85 isolates (44%). Septic shock was identified in 43% of bacteremic patients with type 3 secretion system+ isolates compared to 23% of patients with type 3 secretion system- isolates (p = .12). A high frequency of resistance in the type 3 secretion system+ isolates was observed to ciprofloxacin (59%), cefepime (35%), and gentamicin (38%). There was a significant difference in the 30-day cumulative probability of death after bacteremia between secretors and nonsecretors (p = .02). None of the type 3 secretion system+ patients who survived the first 30 days had a P. aeruginosa isolate which exhibited ExoU phenotype.
Conclusions: The expression of type 3 secretion system exotoxins in bacteremic isolates of P. aeruginosa confers poor clinical outcomes independent of antibiotic susceptibility profile.
Figures
Comment in
-
Pseudomonas aeruginosa bacteremia: targeting virulent phenotypes?Crit Care Med. 2012 Apr;40(4):1354-5. doi: 10.1097/CCM.0b013e31823c8b55. Crit Care Med. 2012. PMID: 22425839 No abstract available.
References
-
- Wisplinghoff H, Bischoff T, Tallent SM, et al. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis. 2004;39(3):309–317. - PubMed
-
- Pittet D, Harbarth S, Ruef C, et al. Prevalence and risk factors for nosocomial infections in four university hospitals in Switzerland. Infect Control Hosp Epidemiol. 1999;20(1):37–42. - PubMed
-
- Kim JM, Park ES, Jeong JS, et al. Multicenter surveillance study for nosocomial infections in major hospitals in Korea. Nosocomial Infection Surveillance Committee of the Korean Society for Nosocomial Infection Control. Am J Infect Control. 2000;28(6):454–458. - PubMed
-
- Vidal F, Mensa J, Almela M, et al. Epidemiology and outcome of Pseudomonas aeruginosa bacteremia, with special emphasis on the influence of antibiotic treatment. Analysis of 189 episodes. Arch Intern Med. 1996;156(18):2121–2126. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
