

Fast-track programmes for hepatopancreatic resections: where do we stand?
- PMID: 22081917
- PMCID: PMC3244621
- DOI: 10.1111/j.1477-2574.2011.00391.x
Fast-track programmes for hepatopancreatic resections: where do we stand?
Abstract
Background: Fast-track (FT) programmes represent a series of multimodal concepts that may reduce surgical stress and speed up convalescence after surgery. The aim of this systematic review was to evaluate FT programmes for patients undergoing hepatopancreatic surgery.
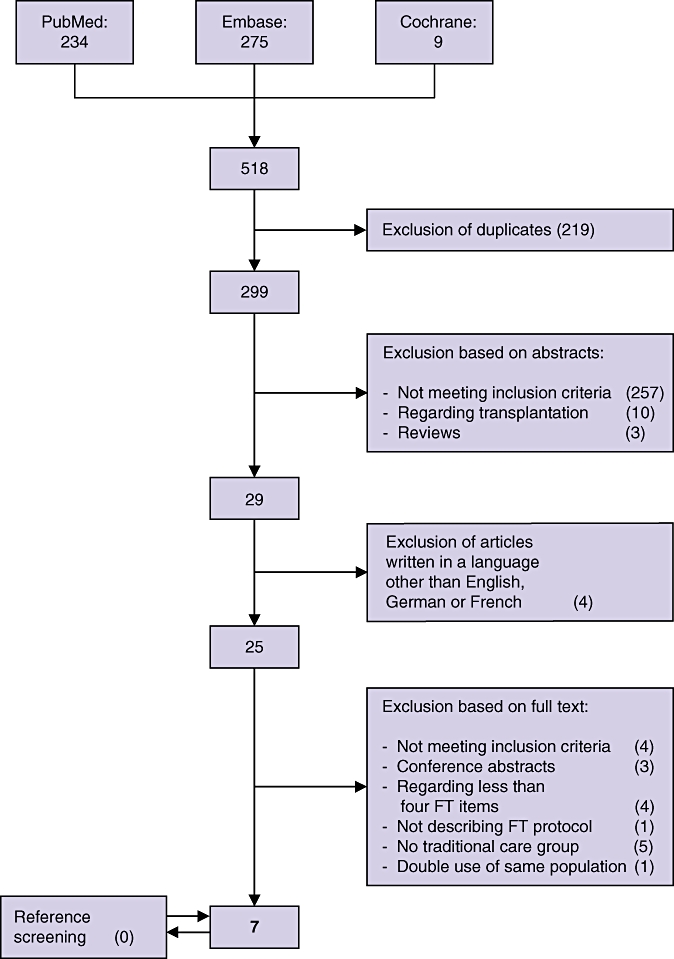
Methods: PubMed, Embase and the Cochrane Library databases were searched for studies of FT vs. conventional recovery strategies for liver and pancreatic resections.
Results: For liver surgery, three cohort studies were included. Primary hospital stay was significantly reduced after FT care in two of the three studies. There were no significant differences in rates of readmission, morbidity and mortality. For pancreatic surgery, three cohort studies and one case-control study were included. Primary hospital stay was significantly shorter after FT care in three out of the four studies. One study reported a significantly decreased readmission rate (7% vs. 25%; P= 0.027), and another study showed lower morbidity (47.2% vs. 58.7%; P < 0.01) in favour of the FT group. There was no difference in mortality between the FT and control groups.
Conclusions: FT rehabilitation for liver and pancreatic surgical patients is feasible. Future investigation should focus on optimizing individual elements of the FT programme within the context of liver and pancreatic surgery.
© 2011 International Hepato-Pancreato-Biliary Association.
References
-
- Varadhan KK, Lobo DN, Ljungqvist O. Enhanced recovery after surgery: the future of improving surgical care. Crit Care Clin. 2010;26:527–547. - PubMed
-
- Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78:606–617. - PubMed
-
- Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg. 2002;183:630–641. - PubMed
-
- Lassen K, Soop M, Nygren J, Cox PB, Hendry PO, Spies C, et al. Consensus review of optimal perioperative care in colorectal surgery: enhanced Recovery After Surgery (ERAS) Group recommendations. Arch Surg. 2009;144:961–969. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
