

Ki67, chemotherapy response, and prognosis in breast cancer patients receiving neoadjuvant treatment
- PMID: 22081974
- PMCID: PMC3262864
- DOI: 10.1186/1471-2407-11-486
Ki67, chemotherapy response, and prognosis in breast cancer patients receiving neoadjuvant treatment
Abstract
Background: The pathological complete response (pCR) after neoadjuvant chemotherapy is a surrogate marker for a favorable prognosis in breast cancer patients. Factors capable of predicting a pCR, such as the proliferation marker Ki67, may therefore help improve our understanding of the drug response and its effect on the prognosis. This study investigated the predictive and prognostic value of Ki67 in patients with invasive breast cancer receiving neoadjuvant treatment for breast cancer.
Methods: Ki67 was stained routinely from core biopsies in 552 patients directly after the fixation and embedding process. HER2/neu, estrogen and progesterone receptors, and grading were also assessed before treatment. These data were used to construct univariate and multivariate models for predicting pCR and prognosis. The tumors were also classified by molecular phenotype to identify subgroups in which predicting pCR and prognosis with Ki67 might be feasible.
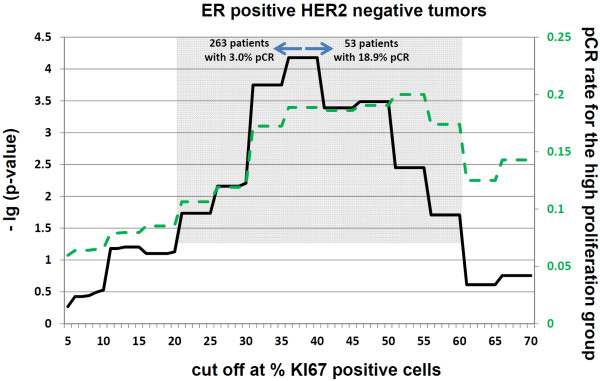
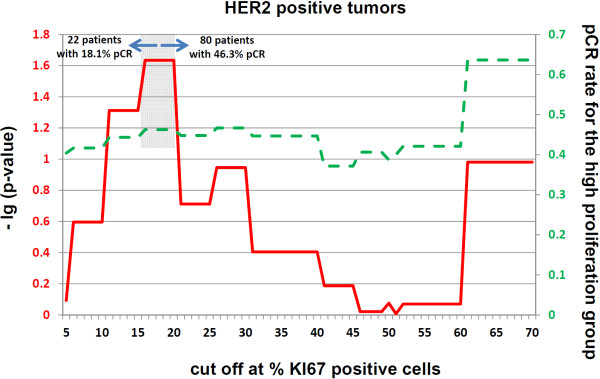
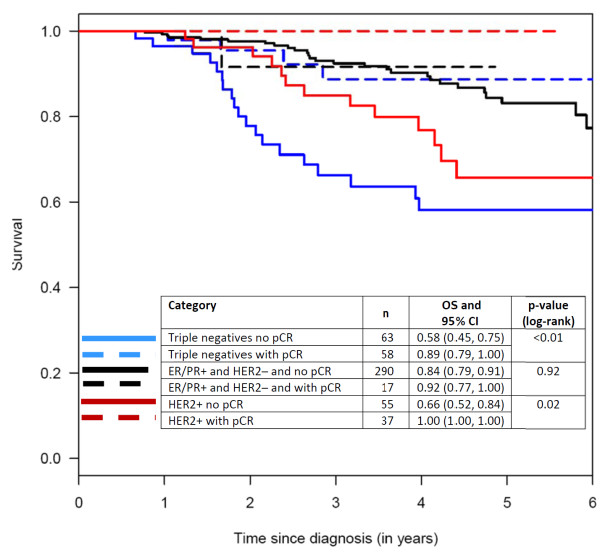
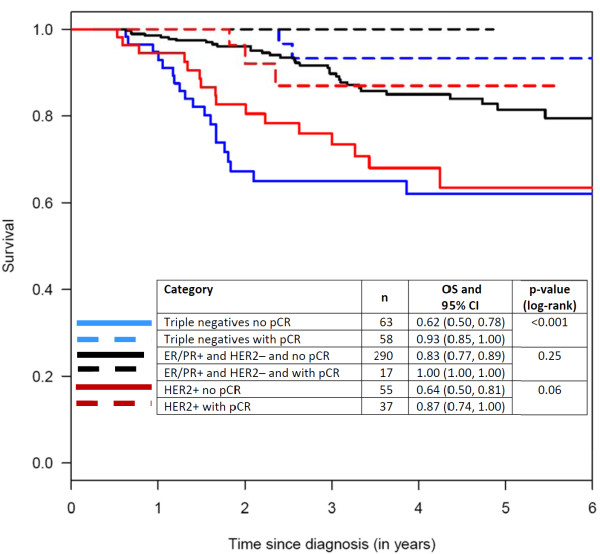
Results: Using a cut-off value of > 13% positively stained cancer cells, Ki67 was found to be an independent predictor for pCR (OR 3.5; 95% CI, 1.4, 10.1) and for overall survival (HR 8.1; 95% CI, 3.3 to 20.4) and distant disease-free survival (HR 3.2; 95% CI, 1.8 to 5.9). The mean Ki67 value was 50.6 ± 23.4% in patients with pCR. Patients without a pCR had an average of 26.7 ± 22.9% positively stained cancer cells.
Conclusions: Ki67 has predictive and prognostic value and is a feasible marker for clinical practice. It independently improved the prediction of treatment response and prognosis in a group of breast cancer patients receiving neoadjuvant treatment. As mean Ki67 values in patients with a pCR were very high, cut-off values in a high range above which the prognosis may be better than in patients with lower Ki67 values may be hypothesized. Larger studies will be needed in order to investigate these findings further.
Figures




References
-
- Paik S, Shak S, Tang G, Kim C, Baker J, Cronin M, Baehner FL, Walker MG, Watson D, Park T, Hiller W, Fisher ER, Wickerham DL, Bryant J, Wolmark N. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004;351:2817–2826. doi: 10.1056/NEJMoa041588. - DOI - PubMed
-
- Harbeck N, Salem M, Nitz U, Gluz O, Liedtke C. Personalized treatment of early-stage breast cancer: present concepts and future directions. Cancer Treat Rev. 2010. - PubMed
-
- Cuzick J, Dowsett M, Wale C, Salter J, Quinn E, Zabaglo L, Howell A, Buzdar A, Forbes JF. Prognostic value of a combined ER, PgR, Ki67, HER2 immunohistochemical (IHC4) score and comparison with the GHI recurrence score -- results from TransATAC. Cancer Res. 2009;69:503s.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
