

Efavirenz pharmacokinetics during the third trimester of pregnancy and postpartum
- PMID: 22083071
- PMCID: PMC3288559
- DOI: 10.1097/QAI.0b013e31823ff052
Efavirenz pharmacokinetics during the third trimester of pregnancy and postpartum
Abstract
Background: The impact of pregnancy on efavirenz (EFV) pharmacokinetics is unknown.
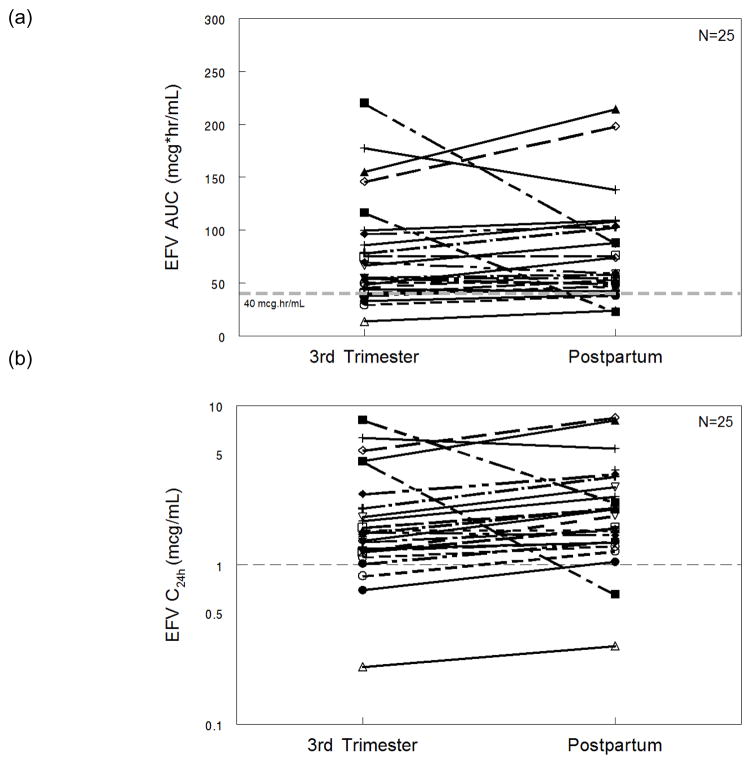
Methods: International Maternal Pediatric Adolescent AIDS Clinical Trials P1026s is an on-going, prospective, nonblinded study of antiretroviral pharmacokinetics in HIV-infected pregnant women that included a cohort receiving 600 mg EFV once daily as part of combination antiretroviral therapy. Intensive steady-state 24-hour blood sampling was performed during the third trimester and at 6-12 weeks postpartum. Maternal and umbilical cord blood samples were drawn at delivery. Pharmacokinetics targets were the estimated 10th percentile EFV area under the curve (AUC) in nonpregnant historical controls (40.0 mcg·hr(-1)·mL(-1)) and a trough concentration of 1 mcg/mL.
Results: Twenty-five women were enrolled during the third trimester: median (range) age was 29.3 (18.9-42.9) years, weight 69.0 (40-130) kg, and gestational age 32.9 (30.1-38.7) weeks. Median (range) EFV AUC(0-24), C(max), and C(24 hours) were 55.4 mcg·hr(-1)·mL(-1) (13.5-220.3), 5.4 mcg/mL (1.9-12.2), and 1.6 mcg/mL (0.23-8.13), respectively. EFV AUC and C(max) did not differ during pregnancy and postpartum but C(24 hours) was lower during the third trimester (1.6 vs. 2.1 mcg/mL, P = 0.01). During the third trimester, 5 of 25 (20%) women had an EFV AUC below the target and 3 of 25 (12%) had a trough concentration below 1 mcg/mL. EFV cord blood/maternal concentration ratio was 0.49 (0.37-0.74). All women had a HIV-1 RNA viral load less than 400 copies per milliliter at delivery and 19 (76%) had a viral load below 50 copies per milliliter. One child was perinatally HIV infected. Three women were exposed to EFV throughout the first 6 weeks of pregnancy. EFV was well tolerated, and among the 25 infants, no congenital anomalies or newborn complications were reported.
Conclusions: Changes in EFV pharmacokinetics during pregnancy compared with postpartum are not sufficiently large enough to warrant a dose adjustment during pregnancy.
Conflict of interest statement
Conflicts of Interest: None Reported
Figures


References
-
- De Santis M, Carducci B, De Santis L, Cavaliere AF, Straface G. Periconceptional exposure to efavirenz and neural tube defects. Arch Intern Med. 2002;162:355. - PubMed
-
- Fundaro C, Genovese O, Rendeli C, Tamburrini E, Salvaggio E. Myelomeningocele in a child with intrauterine exposure to efavirenz. Aids. 2002;16:299–300. - PubMed
-
- Developed by the DHHS Panel on Antiretroviral Guidelines for Adults and Adolescents – A Working Group of the Office of AIDS Research Advisory Council. AIDSinfo; Jan 10, 2011. Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents. Web site ( http://aidsinfonihgov)
-
- Ward BA, Gorski JC, Jones DR, Hall SD, Flockhart DA, Desta Z. The cytochrome P450 2B6 (CYP2B6) is the main catalyst of efavirenz primary and secondary metabolism: implication for HIV/AIDS therapy and utility of efavirenz as a substrate marker of CYP2B6 catalytic activity. J Pharmacol Exp Ther. 2003;306:287–300. - PubMed
-
- Tracy TS, Venkataramanan R, Glover DD, Caritis SN. Temporal changes in drug metabolism (CYP1A2, CYP2D6 and CYP3A Activity) during pregnancy. Am J Obstet Gynecol. 2005;192:633–639. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
