

Practice Guideline
. 2011 Dec;128 Suppl 5(Suppl 5):S213-56.
doi: 10.1542/peds.2009-2107C.
Epub 2011 Nov 14.
Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report
- PMID: 22084329
- PMCID: PMC4536582
- DOI: 10.1542/peds.2009-2107C
Item in Clipboard
Practice Guideline
Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report
Pediatrics.
2011 Dec.
No abstract available
Figures
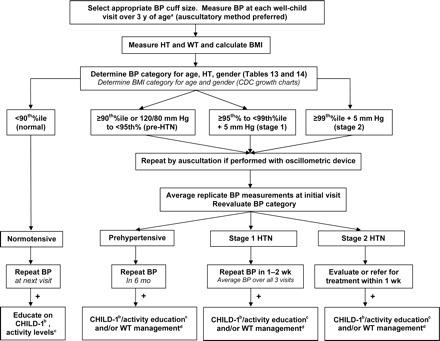
BP measurement and categorization. HT indicates height; WT, weight; HTN, hypertension; %ile, percentile. a See Table 8-2; b see “Nutrition and Diet”Table 5-1; c see “Physical Activity”; c see “Overweight and Obesity.” Adapted from High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. Pediatrics. 2004;114(2 suppl 4th report):555–576.

BP management according to category. HTN indicates hypertension; CV, cardiovascular; Hx, history; PEx, physical examination; CBC, complete blood count; U/A, urinalysis; U/S, ultrasound; Ped, pediatric; LVH, left ventricular hypertrophy; Q, every; Rx, prescription; 2°, secondary; W/U, workup; TOD, target organ damage; s/p, status post; CKD, chronic kidney disease; %ile, percentile. a Workup for target organ damage/left ventricular hypertrophy if obese or positive for other cardiovascular risk factors; b see “Nutrition and Diet”; c see “Physical Activity”; d see “Overweight and Obesity.” Adapted from High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. Pediatrics. 2004;114(2 suppl 4th report):555–576.

Dyslipidemia algorithm: target LDL cholesterol. Values given are in mg/dL. To convert to SI units, divide results for TC, LDL cholesterol, HDL cholesterol, and non-HDL cholesterol by 38.6; for triglycerides, divide by 88.6. TG indicates triglycerides; C, cholesterol; RF, risk factor; FHx, family history; a Obtain FLPs at least 2 weeks but no more than 3 months apart. b Per Table 9-9, use of drug therapy is limited to children aged 10 years and older with defined risk profiles. c In a child with an LDL cholesterol level of >190 mg/dL and other risk factors, a trial of the CHILD-2–LDL may be abbreviated.
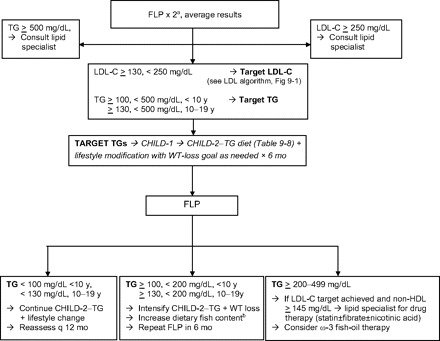
Dyslipidemia algorithm: target triglycerides. Values given are in mg/dL. To convert to SI units, divide results for TC, LDL cholesterol, HDL cholesterol, and non-HDL cholesterol by 38.6; for triglycerides, divide by 88.6. C indicates cholesterol; a Obtain FLPs at least 2 weeks but no more than 3 months apart. b The FDA and the Environmental Protection Agency advise women of childbearing age who may become pregnant, pregnant women, nursing mothers, and young children to avoid some types of fish and shellfish and to eat fish and shellfish that are lower in mercury. For more information, call the FDA's food information line toll-free at 1-888-SAFEFOOD or visit www.cfsan.fda.gov/∼dms/admehg3.html .
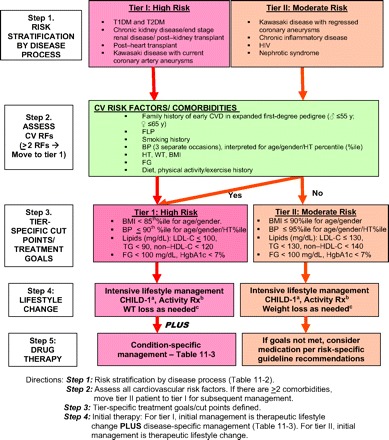
Risk stratification and management for children with conditions predisposing to accelerated atherosclerosis and early CVD. CV indicates cardiovascular; RF, risk factor; HT, height; WT, weight; TG, triglycerides; %ile, percentile; C, cholesterol; FG, fasting glucose; Rx, recommendation. a See “Nutrition and Diet”; b see “Physical Activity”; c see “Overweight and Obesity.” Adapted from Kavey RE, Allada V, Daniels SR, et al; American Heart Association, Expert Panel on Population and Prevention Science; American Heart Association, Council on Cardiovascular Disease in the Young; American Heart Association, Council on Epidemiology and Prevention; American Heart Association, Council on Nutrition, Physical Activity and Metabolism; American Heart Association, Council on High Blood Pressure Research; American Heart Association, Council on Cardiovascular Nursing; American Heart Association, Council on the Kidney in Heart Disease; Interdisciplinary Working Group on Quality of Care and Outcomes Research. Circulation. 2006;114(24):2710–2738.
References
-
- NCEP Expert Panel of Blood Cholesterol Levels in Children and Adolescents. National Cholesterol Education Program (NCEP): highlights of the report of the Expert Panel on Blood Cholesterol Levels in Children and Adolescents. Pediatrics. 1992;89(3):495–501 - PubMed
-
- Strong JP, Malcom GT, McMahan CA, et al. ; Prevalence and extent of atherosclerosis in adolescents and young adults: implications for prevention from the Pathobiological Determinants of Atherosclerosis in Youth Study. JAMA. 1999;281(3):495–501 - PubMed
-
- Berenson GS, Srinivasan SR, Bao W, Newman WP, III, Tracy RE, Wattigney WA. Association between multiple cardiovascular risk factors and atherosclerosis in children and young adults. The Bogalusa Heart Study. N Engl J Med. 1998;338(23):1650–1656 - PubMed
-
- Morrison JA, Friedman LA, Gray-McGuire C. Metabolic syndrome in childhood predicts adult cardiovascular disease 25 years later: the Princeton Lipid Research Clinics Follow-up Study. Pediatrics. 2007;120(2):340–345 - PubMed
-
- McMahan CA, Gidding SS, Malcolm GT, et al. Pathobiological Determinants of Atherosclerosis in Youth (PDAY) Research Group. Comparison of coronary heart disease risk factors in autopsied young adults from the PDAY Study with living young adults from the CARDIA study. Cardiovasc Pathol. 2007;16(3):151–158 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
