

Novel staging system for predicting disease-specific survival in patients with breast cancer treated with surgery as the first intervention: time to modify the current American Joint Committee on Cancer staging system
- PMID: 22084362
- PMCID: PMC3236648
- DOI: 10.1200/JCO.2011.38.3174
Novel staging system for predicting disease-specific survival in patients with breast cancer treated with surgery as the first intervention: time to modify the current American Joint Committee on Cancer staging system
Abstract
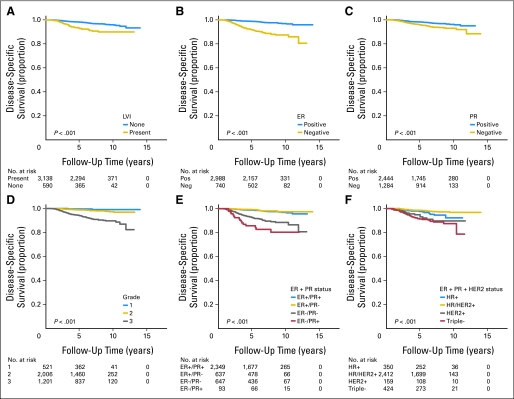
Purpose: American Joint Committee on Cancer (AJCC) staging is used to determine breast cancer prognosis, yet patient survival within each stage shows wide variation. We hypothesized that differences in biology influence this variation and that addition of biologic markers to AJCC staging improves determination of prognosis.
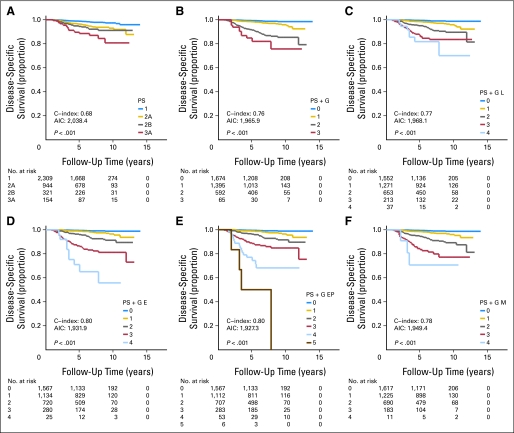
Patients and methods: We identified a cohort of 3,728 patients who underwent surgery as the first intervention between 1997 and 2006. A Cox proportional hazards model, with backward stepwise exclusion of factors and stratification on pathologic stage (PS), was used to test the significance of adding grade (G), lymphovascular invasion (L), estrogen receptor (ER) status (E), progesterone receptor (PR) status, combined ER and PR status (EP), or combined ER, PR, and human epidermal growth factor receptor 2 status (M). We assigned values of 0 to 2 to these disease-specific survival (DSS) -associated factors and assessed six different staging systems: PS, PS + G, PS + G L, PS + G E, PS + G EP, and PS + G M. We compared 5-year DSS rates, Akaike's information criterion (AIC), and Harrell's concordance index (C-index) between systems. Surveillance, Epidemiology, and End Results data were used as the external validation cohort (n = 26,711).
Results: Median follow-up was 6.5 years, and 5-year DSS rate was 97.4%. The PS + G E status staging system was most precise, with a low AIC (1,931.9) and the highest C-index (0.80). PS + G E status was confirmed to stratify outcomes in internal bootstrapping samples and the external validation cohort.
Conclusion: Our results validate an improved breast cancer staging system that incorporates grade and ER status. We recommend that biologic markers be incorporated into revised versions of the AJCC staging system.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures

References
-
- Edge SB, Byrd DR, Compton CC. AJCC Cancer Staging Manual. ed 7. Chicago, IL: Springer; 2009.
-
- Elston CW, Ellis IO. Pathological prognostic factors in breast cancer: I. The value of histological grade in breast cancer—Experience from a large study with long-term follow-up. Histopathology. 1991;19:403–410. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
