

Surgical brain metastases: management and outcome related to prognostic indexes: a critical review of a ten-year series
- PMID: 22084749
- PMCID: PMC3195773
- DOI: 10.5402/2011/207103
Surgical brain metastases: management and outcome related to prognostic indexes: a critical review of a ten-year series
Abstract
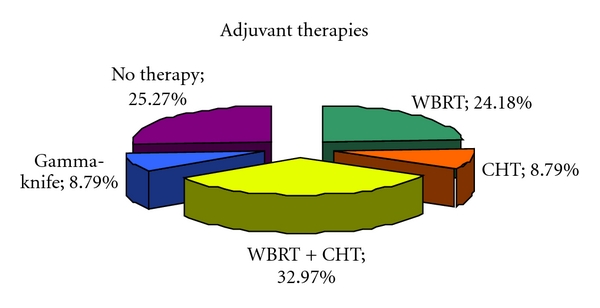
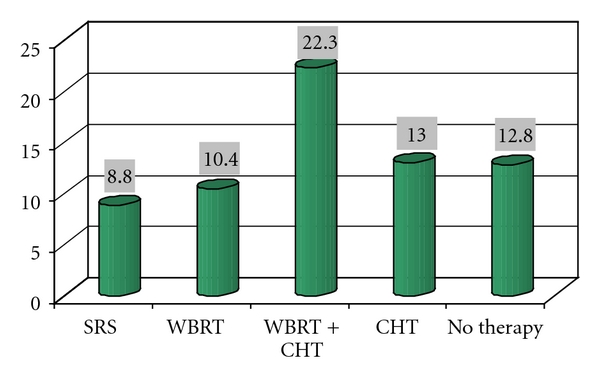
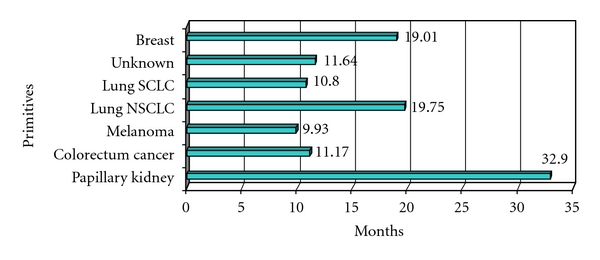
Brain metastasis are the most common neoplastic lesions of the nervous system. Many cancer patients are diagnosed on the basis of a first clinical presentation of cancer on the basis of a single or multiple brain lesions. Brain metastases are manifestations of primary disease progression and often determine a poor prognosis. Not all patients with a brain metastases undergo surgery: many are submitted to alternative or palliative treatments. Management of patients with brain metastases is still controversial, and many studies have been developed to determine which is the best therapy. Furthermore, management of patients operated for a brain metastasis is often difficult. Chemotherapy, stereotactic radiosurgery, panencephalic radiation therapy, and surgery, in combination or alone, are the means most commonly used. We report our experience in the management of a ten-year series of surgical brain metastasis and discuss our results in the preoperative and postoperative management of this complex condition.
Figures
References
-
- Al-Shamy G, Sawaya R. Management of brain metastases: the indispensable role of surgery. Journal of Neuro-Oncology. 2009;92(3):275–282. - PubMed
-
- Barker FG., II Surgical and radiosurgical management of brain metastases. Surgical Clinics of North America. 2005;85(2):329–345. - PubMed
-
- Soffietti R, Rudà R, Trevisan E. Brain metastases: current management and new developments. Current Opinion in Oncology. 2008;20(6):676–684. - PubMed
-
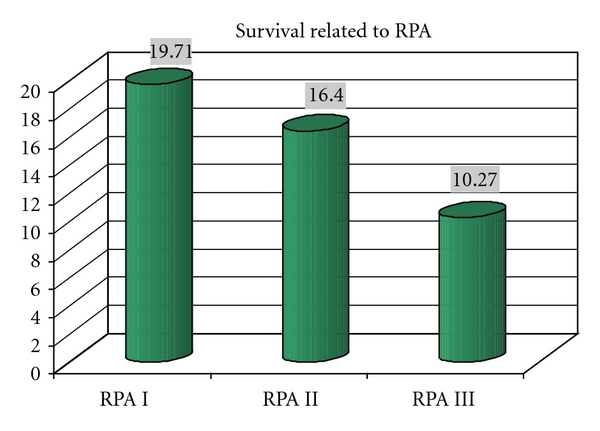
- Gaspar L, Scott C, Rotman M, et al. Recursive Partitioning Analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. International Journal of Radiation Oncology Biology Physics. 1997;37(4):745–751. - PubMed
LinkOut - more resources
Full Text Sources