

Noninvasive assessment of liver fibrosis with the aspartate transaminase to platelet ratio index (APRI): Usefulness in patients with chronic liver disease: APRI in chronic liver disease
- PMID: 22087126
- PMCID: PMC3206675
Noninvasive assessment of liver fibrosis with the aspartate transaminase to platelet ratio index (APRI): Usefulness in patients with chronic liver disease: APRI in chronic liver disease
Abstract
Background: The aspartate aminotransferases (AST) to platelet ratio index (APRI) may serve as a noninvasive marker to assess liver fibrosis.
Objectives: To assess the diagnostic ability of the APRI for prediction of fibrosis in patients with chronic hepatitis B (CHB), chronic hepatitis C (CHC), and non-alcoholic fatty liver disease (NAFLD).
Patients and methods: This retrospective study included 207 patients with CHB, 108 with CHC, and 140 patients with NAFLD. The APRI was calculated as (AST level/upper normal limit for AST)/platelet counts (109/L) × 100. The stage of liver fibrosis in patients with chronic viral hepatitis was graded using the METAVIR scale. The Kleiner system for grading fibrosis was used in patients with NAFLD.
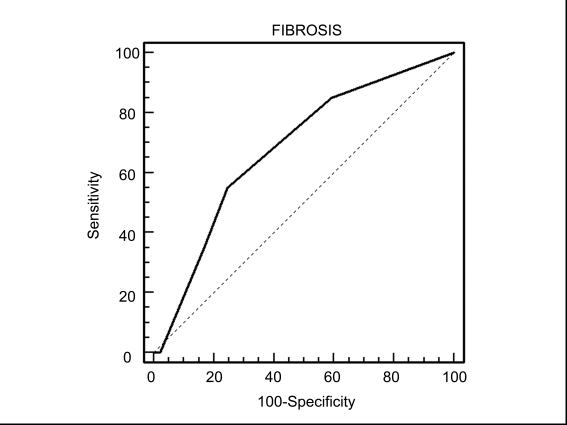
Results: Bivariate correlation analyses showed that the APRI was significantly associated with fibrosis scores in patients with CHC (p = 0.2634, p = 0.0059) and NAFLD (p = 0.2273, p = 0.0069), but not in those with CHB (p = 0.1005, p = 0.1495). Receiver operating characteristic (ROC) curves were used for assessing the ability of the APRI as a predictor of the absence or presence of liver fibrosis (fibrosis score of 0 vs fibrosis scores of 1-4). In patients with CHC, the APRI showed a sensitivity of 72.7% and a specificity of 62.4% for detection of fibrosis (p<0.01). In the NAFLD group, the APRI showed a sensitivity of 60.0% and specificity of 73.3% for detection of fibrosis (p<0.01). In patients with CHB, the APRI showed a sensitivity of 55.0% and a specificity of 75.4% for fibrosis (p=NS).
Conclusions: The APRI shows an acceptable accuracy for the assessment of liver fibrosis in patients with CHC and NAFLD, but not in those with CHB.
Keywords: Aspartate aminotransferases; Chronic hepatitis B; Chronic hepatitis C; Fatty liver; Fibrosis.
Figures


References
-
- Iredale J. Defining therapeutic targets for liver fibrosis: exploiting the biology of inflammation and repair. Pharmacol Res. 2008;58(2):129–36. - PubMed
-
- Denzer UW, Luth S. Non-invasive diagnosis and monitoring of liver fibrosis and cirrhosis. Best Pract Res Clin Gastroenterol. 2009;23(3):453–60. - PubMed
-
- Castera L. Assessing liver fibrosis. Expert Rev Gastroenterol Hepatol. 2008;(4):541–52. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous