

Treatment and prevention of urinary tract infection with orally active FimH inhibitors
- PMID: 22089451
- PMCID: PMC3694776
- DOI: 10.1126/scitranslmed.3003021
Treatment and prevention of urinary tract infection with orally active FimH inhibitors
Abstract
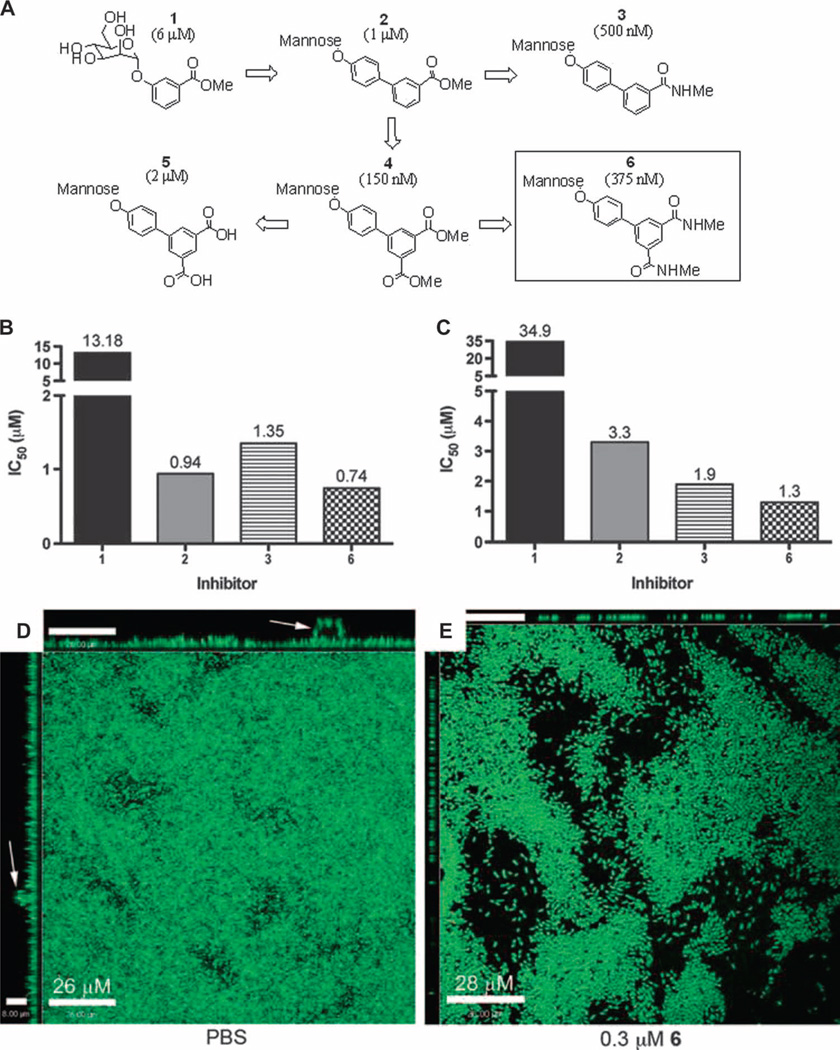
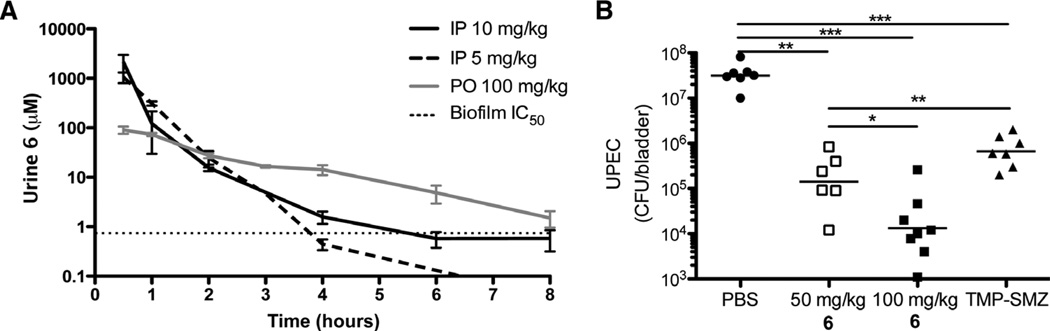
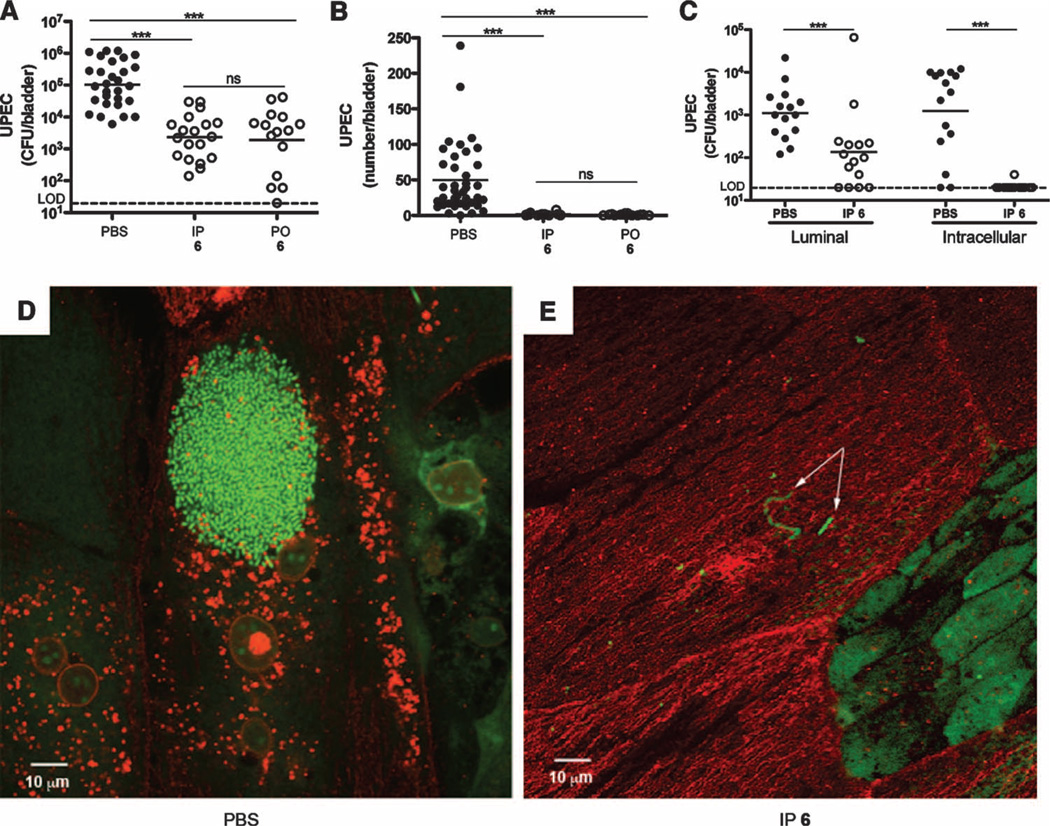
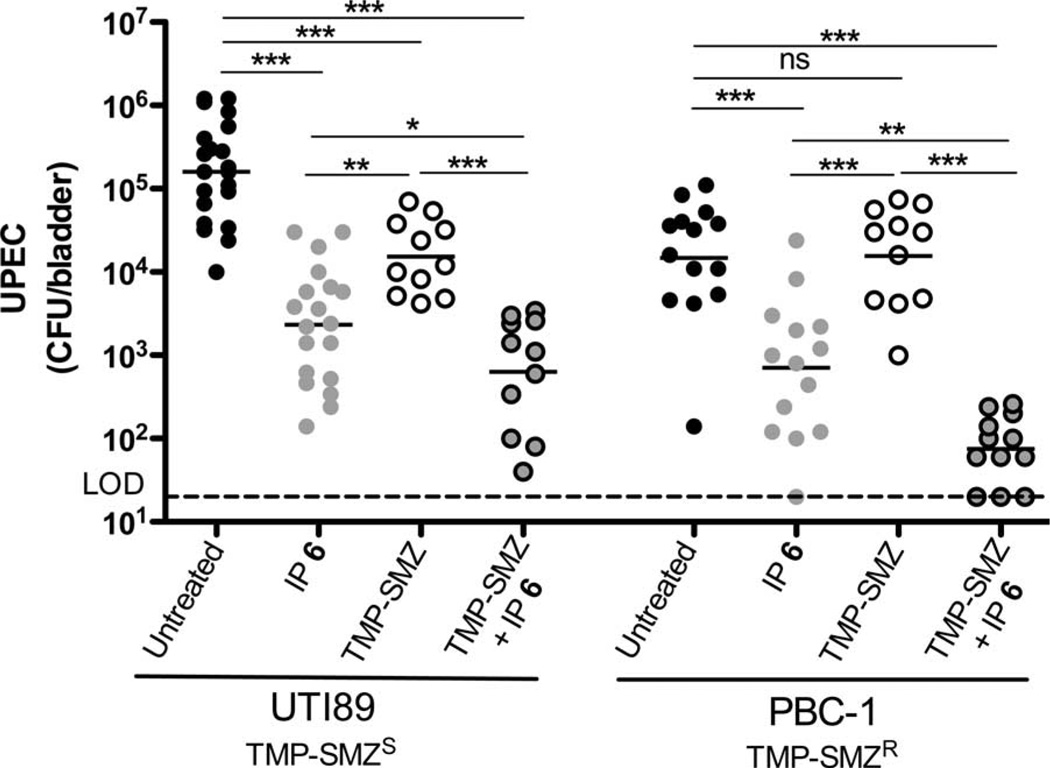
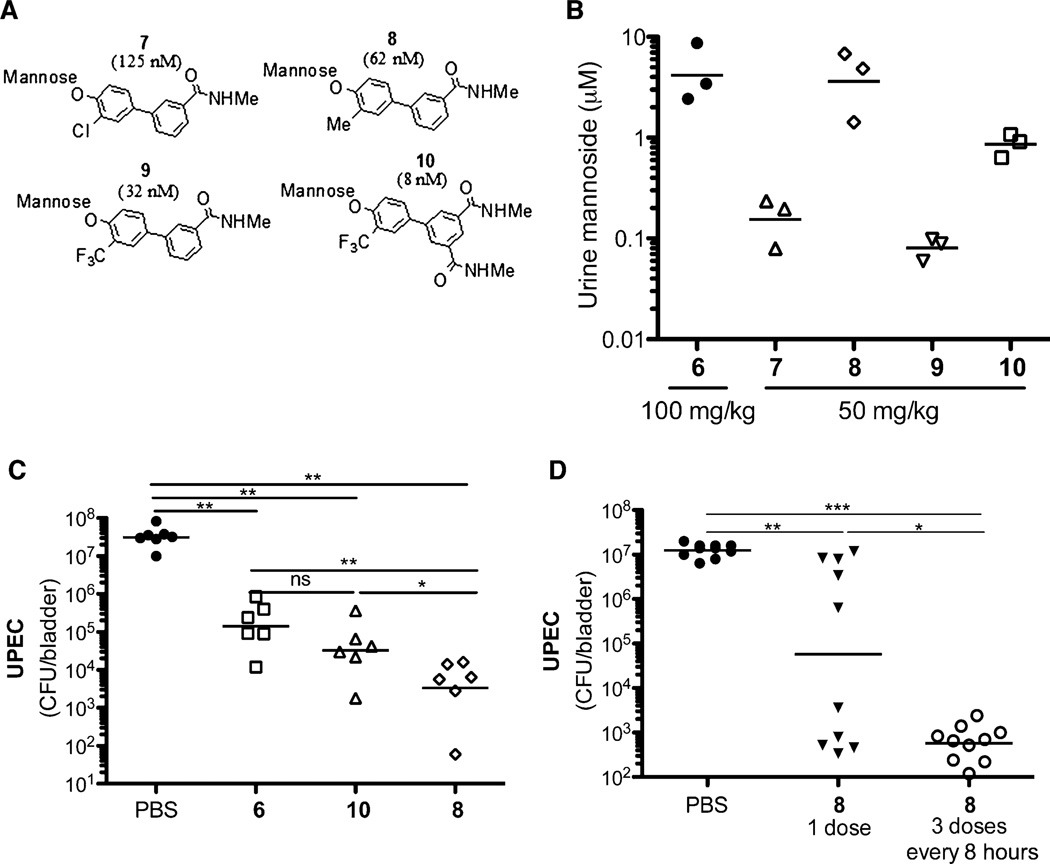
Chronic and recurrent urinary tract infections pose a serious medical problem because there are few effective treatment options. Patients with chronic urinary tract infections are commonly treated with long-term prophylactic antibiotics that promote the development of antibiotic-resistant forms of uropathogenic Escherichia coli (UPEC), further complicating treatment. We developed small-molecular weight compounds termed mannosides that specifically inhibit the FimH type 1 pilus lectin of UPEC, which mediates bacterial colonization, invasion, and formation of recalcitrant intracellular bacterial communities in the bladder epithelium. Here, we optimized these compounds for oral bioavailability and demonstrated their fast-acting efficacy in treating chronic urinary tract infections in a preclinical murine model. These compounds also prevented infection in vivo when given prophylactically and strongly potentiated the activity of the current standard of care therapy, trimethoprim-sulfamethoxazole, against clinically resistant PBC-1 UPEC bacteria. These compounds have therapeutic efficacy after oral administration for the treatment of established urinary tract infections in vivo. Their unique mechanism of action-targeting the pilus tip adhesin FimH-circumvents the conventional requirement for drug penetration of the outer membrane, minimizing the potential for the development of resistance. The small-molecular weight compounds described herein promise to provide substantial benefit to women suffering from chronic and recurrent urinary tract infections.
Figures
Comment in
-
Urinary tract infections: oral FimH inhibitors effective against UTI.Nat Rev Urol. 2011 Dec 27;9(1):6. doi: 10.1038/nrurol.2011.204. Nat Rev Urol. 2011. PMID: 22200833 No abstract available.
References
-
- Boucher HW, Talbot GH, Bradley JS, Edwards JE, Gilbert D, Rice LB, Scheld M, Spellberg B, Bartlett J. Bad bugs, no drugs: No ESKAPE! An update from the infectious diseases Society of America. Clin. Infect. Dis. 2009;48:1–12. - PubMed
-
- Ubeda C, Taur Y, Jenq RR, Equinda MJ, Son T, Samstein M, Viale A, Socci ND, van den Brink MR, Kamboj M, Pamer EG. Vancomycin-resistant Enterococcus domination of intestinal microbiota is enabled by antibiotic treatment in mice and precedes bloodstream invasion in humans. J. Clin. Invest. 2010;120:4332–4341. - PMC - PubMed
-
- Ho J, Tambyah PA, Paterson DL. Multiresistant Gram-negative infections: A global perspective. Curr. Opin. Infect. Dis. 2010;23:546–553. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R37 AI048689/AI/NIAID NIH HHS/United States
- R01 AI048689/AI/NIAID NIH HHS/United States
- R01 AI049950/AI/NIAID NIH HHS/United States
- P50 DK064540/DK/NIDDK NIH HHS/United States
- P30 DK056341/DK/NIDDK NIH HHS/United States
- AI49950/AI/NIAID NIH HHS/United States
- R01 DK051406/DK/NIDDK NIH HHS/United States
- K12 HD001459/HD/NICHD NIH HHS/United States
- RC1DK086378-02/DK/NIDDK NIH HHS/United States
- P60 DK020579/DK/NIDDK NIH HHS/United States
- DK51406/DK/NIDDK NIH HHS/United States
- P41 RR000954/RR/NCRR NIH HHS/United States
- RC1 DK086378/DK/NIDDK NIH HHS/United States
- AI48689/AI/NIAID NIH HHS/United States
- P60-DK20579/DK/NIDDK NIH HHS/United States
- K12 HD001459-09/HD/NICHD NIH HHS/United States
- DK64540/DK/NIDDK NIH HHS/United States
- P41-RR00954/RR/NCRR NIH HHS/United States
- P30-DK56341/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
