

Gastroschisis: one year outcomes from national cohort study
- PMID: 22089731
- PMCID: PMC3216470
- DOI: 10.1136/bmj.d6749
Gastroschisis: one year outcomes from national cohort study
Abstract
Objective: To describe one year outcomes for a national cohort of infants with gastroschisis.
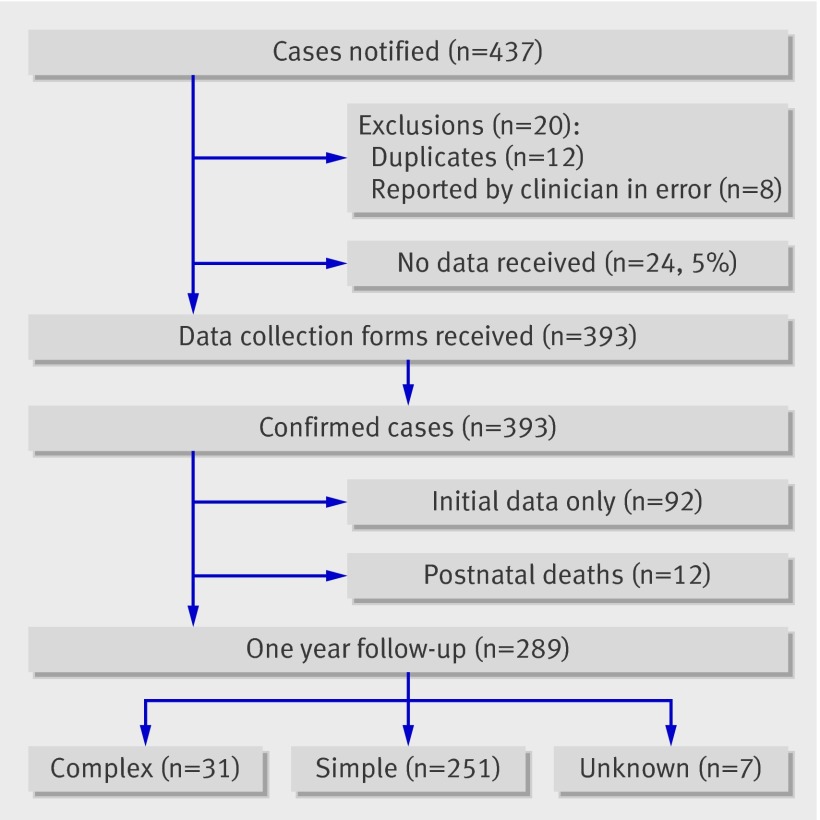
Design: Population based cohort study of all liveborn infants with gastroschisis born in the United Kingdom and Ireland from October 2006 to March 2008.
Setting: All 28 paediatric surgical centres in the UK and Ireland.
Participants: 301 infants (77%) from an original cohort of 393.
Main outcome measures: Duration of parenteral nutrition and stay in hospital; time to establish full enteral feeding; rates of intestinal failure, liver disease associated with intestinal failure, unplanned reoperation; case fatality.
Results: Compared with infants with simple gastroschisis (intact, uncompromised, continuous bowel), those with complex gastroschisis (bowel perforation, necrosis, or atresia) took longer to reach full enteral feeding (median difference 21 days, 95% confidence interval 9 to 39 days); required a longer duration of parenteral nutrition (median difference 25 days, 9 to 46 days) and a longer stay in hospital (median difference 57 days, 29 to 95 days); were more likely to develop intestinal failure (81% (25 infants) v 41% (102); relative risk 1.96, 1.56 to 2.46) and liver disease associated with intestinal failure (23% (7) v 4% (11); 5.13, 2.15 to 12.3); and were more likely to require unplanned reoperation (42% (13) v 10% (24); 4.39, 2.50 to 7.70). Compared with infants managed with primary fascial closure, those managed with preformed silos took longer to reach full enteral feeding (median difference 5 days, 1 to 9) and had an increased risk of intestinal failure (52% (50) v 32% (38); 1.61, 1.17 to 2.24). Event rates for the other outcomes were low, and there were no other significant differences between these management groups. Twelve infants died (4%).
Conclusions: This nationally representative study provides a benchmark against which individual centres can measure outcome and performance. Stratifying neonates with gastroschisis into simple and complex groups reliably predicts outcome at one year. There is sufficient clinical equipoise concerning the initial management strategy to embark on a multicentre randomised controlled trial comparing primary fascial closure with preformed silos in infants suitable at presentation for either treatment to determine the optimal initial management strategy and define algorithms of care.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Gastroschisis.BMJ. 2011 Nov 15;343:d7124. doi: 10.1136/bmj.d7124. BMJ. 2011. PMID: 22089733 No abstract available.
References
-
- Keys C, Drewett M, Burge DM. Gastroschisis: the cost of an epidemic. J Pediatr Surg 2008;43:654-7. - PubMed
-
- Alvarez SM, Burd RS. Increasing prevalence of gastroschisis repairs in the United States: 1996-2003. J Pediatr Surg 2007;42:943-6. - PubMed
-
- European Surveillance of Congenital Anomalies (EUROCAT). EUROCAT report 8: Surveillance of congenital anomalies 1980-1999. EUROCAT Central Registry, University of Ulster, 2001.
-
- Laughon M, Meyer R, Bose C, Wall A, Otero E, Heerens A, et al. Rising birth prevalence of gastroschisis. J Perinatol 2003;23:291-3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical