

Ten-year survival after liver resection for colorectal metastases: systematic review and meta-analysis
- PMID: 22091431
- PMCID: PMC3200144
- DOI: 10.5402/2011/763245
Ten-year survival after liver resection for colorectal metastases: systematic review and meta-analysis
Abstract
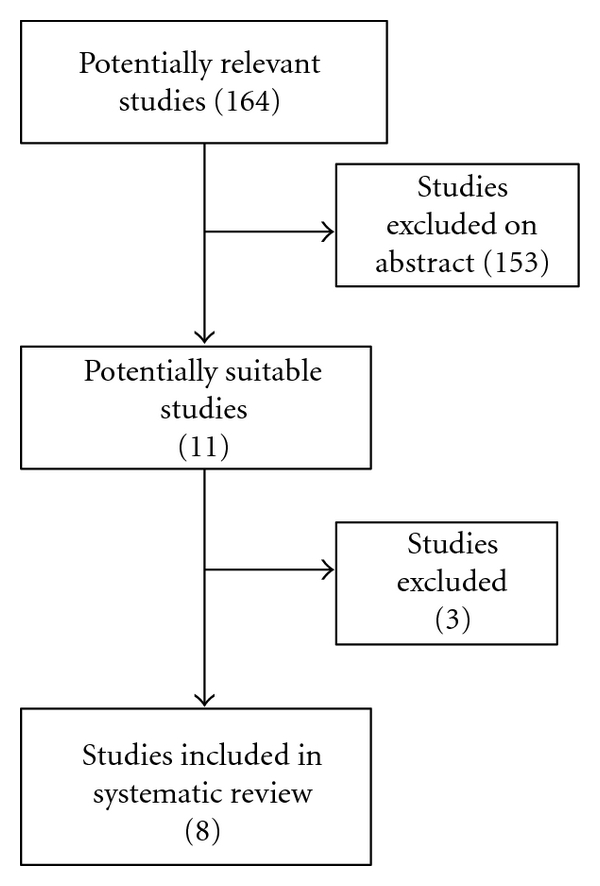
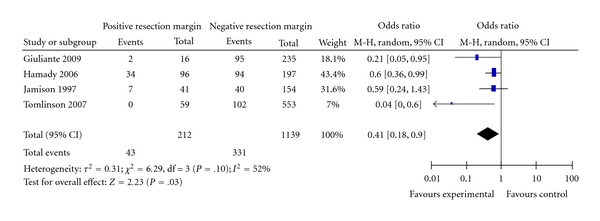
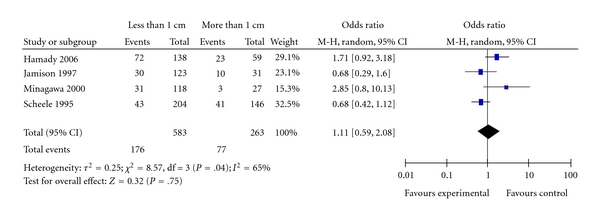
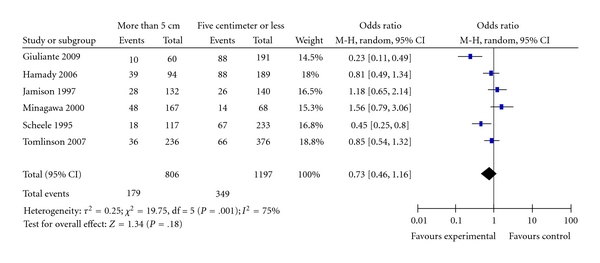
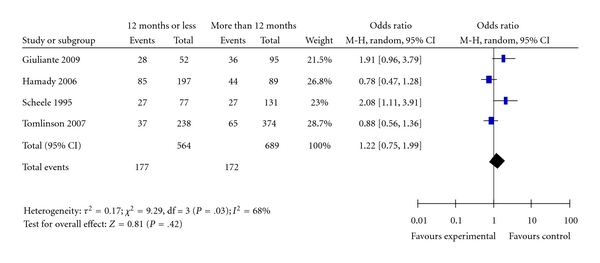
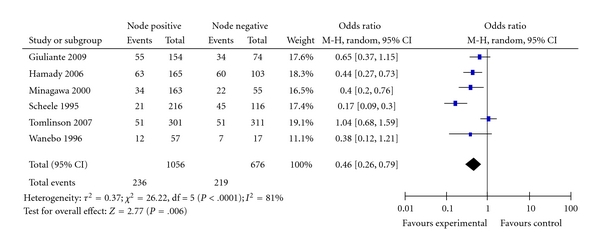
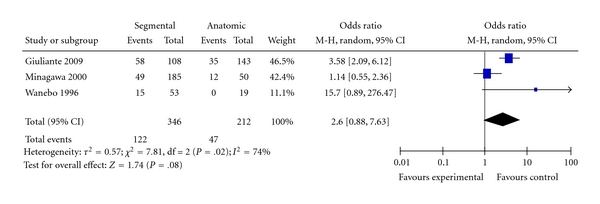
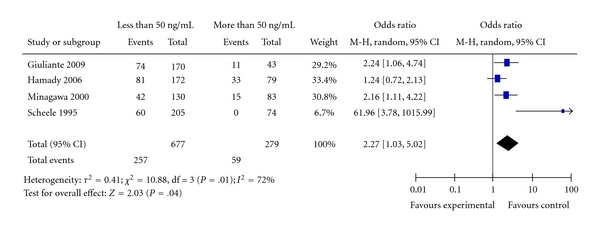
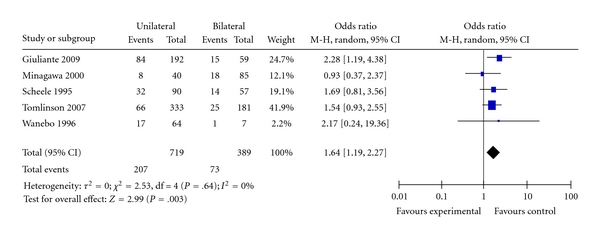
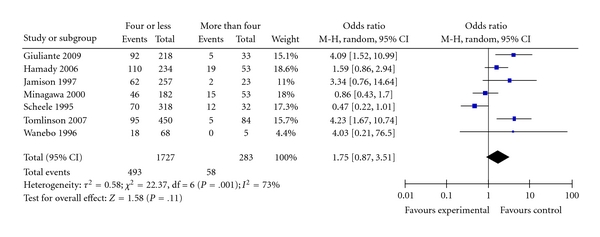
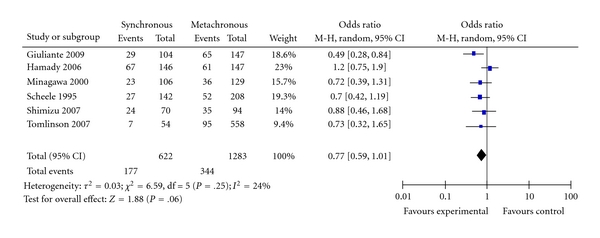
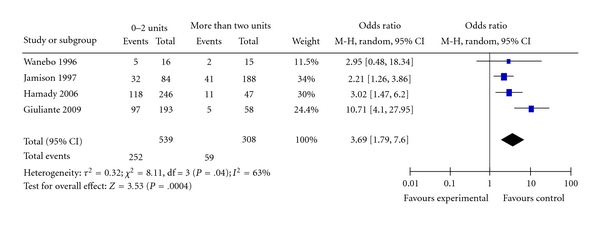
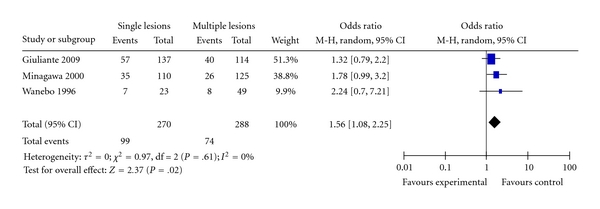
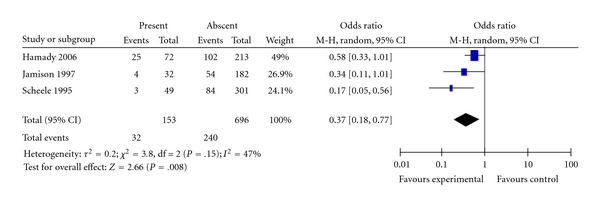
Background. Liver resection in metastatic colorectal cancer is proved to result in five-year survival of 25-40%. Several factors have been investigated to look for prognostic factors stratifications such as resection margins, node involvement in the primary disease, and interval between the primary disease and liver metastases. Methods. We searched MEDLINE and EMBASE for studies that reported ten-year survival. Metaanalysis was performed to analyse the effect of recognised prognostic factors on cure rate for colorectal metastases. The meta-analysis was performed according to Ottawa-Newcastle method of analysis for nonrandomised trials and according to the guidelines of the PRISMA. Results. Eleven studies were included in the analysis, which showed a ten-year survival rate of 12-36%. Factors that have favourable impact are clear resection margin, low level of CEA, single metastatic deposit, and node negative disease. The only factor that excluded patients from cure is the positive status of the resection margin. Conclusion. Predicted ten-year survival after liver resection for colorectal metastases varies from 12 to 36%. Only positive resection margins resulted in no 10-year survivors. No patient can be excluded from consideration for liver resection so long the result is negative margins.
Figures
References
-
- Mackay HJ, Billingsley K, Gallinger S, et al. A multicenter phase II study of “adjuvant” irinotecan following resection of colorectal hepatic metastases. American Journal of Clinical Oncology. 2005;28(6):547–554. - PubMed
LinkOut - more resources
Full Text Sources
