

Vulnerability: the crossroads of frailty and delirium
- PMID: 22091571
- PMCID: PMC3233987
- DOI: 10.1111/j.1532-5415.2011.03674.x
Vulnerability: the crossroads of frailty and delirium
Abstract
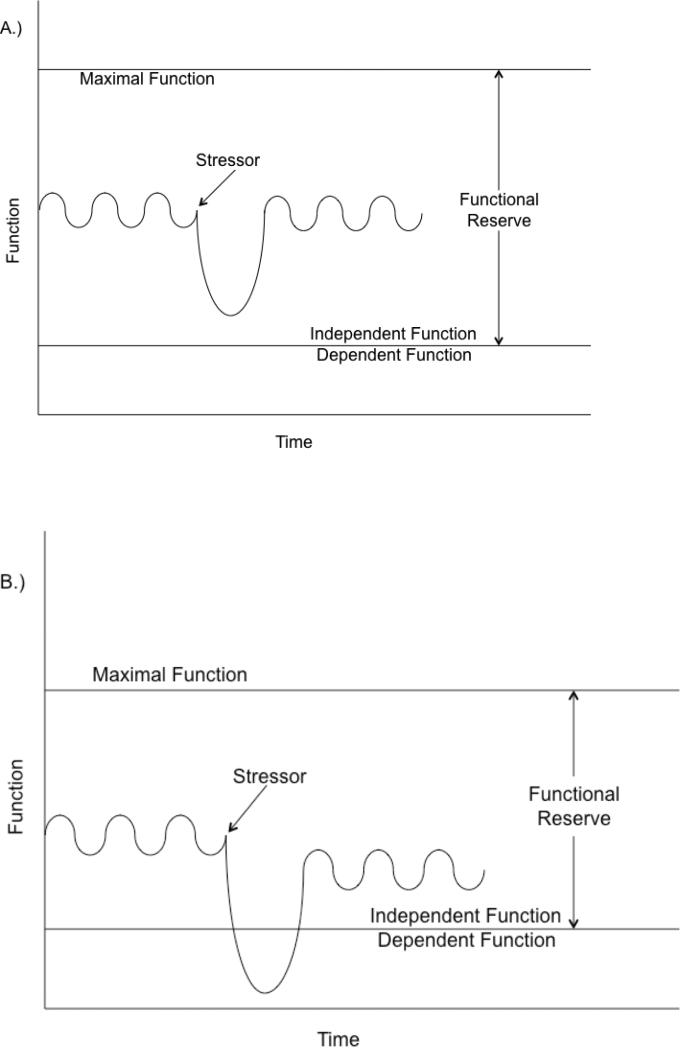
Frailty and delirium, although seemingly distinct syndromes, both result in significant negative health outcomes in older adults. Frailty and delirium may be different clinical expressions of a shared vulnerability to stress in older adults, and future research will determine whether this vulnerability is age related, pathological, genetic, environmental, or most likely, a combination of all of these factors. This article explores the clinical overlap of frailty and delirium, describes possible pathophysiological mechanisms linking the two, and proposes research opportunities to further knowledge of the interrelationships between these important geriatric syndromes. Frailty, a diminished ability to compensate for stressors, is generally viewed as a chronic condition, whereas delirium is an acute change in attention and cognition, but there is a developing literature on transitions in frailty status around acute events, as well as on delirium as a chronic, persistent condition. If frailty predisposes an individual to delirium, and delirium delays recovery from a stressor, then both syndromes may contribute to a downward spiral of declining function, increasing risk, and negative outcomes. In addition, frailty and delirium may have shared pathophysiology, such as inflammation, atherosclerosis, and chronic nutritional deficiencies, which will require further investigation. The fields of frailty and delirium are rapidly evolving, and future research may help to better define the interrelationship of these common and morbid geriatric syndromes. Because of the heterogeneous pathophysiology and presentation associated with frailty and delirium, typical of all geriatric syndromes, multicomponent prevention and treatment strategies are most likely to be effective and should be developed and tested.
© 2011, Copyright the Authors Journal compilation © 2011, The American Geriatrics Society.
Figures
References
-
- Jarrett PG, Rockwood K, Carver D, et al. Cosway S. Illness presentation in elderly patients. Arch Intern Med. 1995;155:1060–1064. - PubMed
-
- Taffet G. Physiology of Aging. In: Cassel C, editor. Geriatric medicine: an evidence-based approach. 4th edN. Springer-Verlag; New York: 2003. pp. 27–35.
-
- Resnick NM, Marcantonio ER. How should clinical care of the aged differ? Lancet. 1997;350:1157–1158. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
