

Periodontal disease, tooth loss and incident rheumatoid arthritis: results from the First National Health and Nutrition Examination Survey and its epidemiological follow-up study
- PMID: 22092471
- PMCID: PMC3403745
- DOI: 10.1111/j.1600-051X.2011.01776.x
Periodontal disease, tooth loss and incident rheumatoid arthritis: results from the First National Health and Nutrition Examination Survey and its epidemiological follow-up study
Abstract
Aims: Infection may be a rheumatoid arthritis (RA) risk factor. We examined whether signs of periodontal infection were associated with RA development in the First National Health and Nutrition Examination Survey and its epidemiological follow-up study.
Material and methods: In 1971-1974, 9702 men and women aged 25-74 were enrolled and surveyed longitudinally (1982, 1986, 1987, 1992). Periodontal infection was defined by baseline tooth loss or clinical evidence of periodontal disease. Baseline (n = 138) and incident (n = 433) RA cases were defined via self-report physician diagnosis, joint pain/swelling, ICD-9 codes (714.0-714.9), death certificates and/or RA hospitalization.
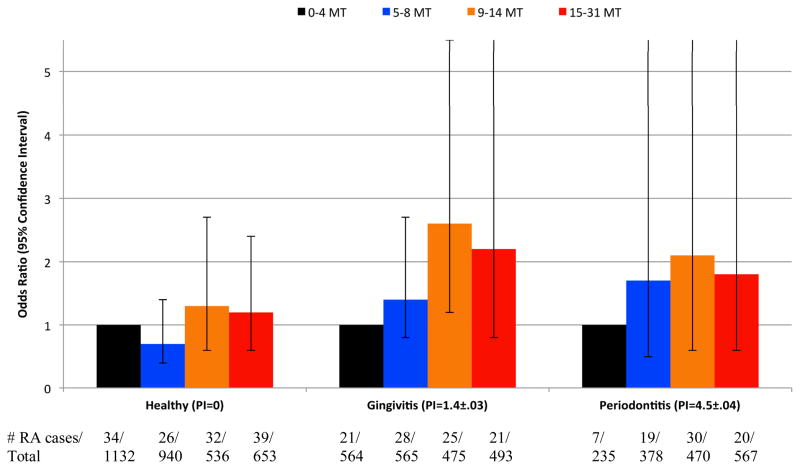
Results: Adjusted odds ratios (ORs) (95% CI) for prevalent RA in gingivitis and periodontitis (versus healthy) were 1.09 (0.57, 2.10) and 1.85 (0.95, 3.63); incident RA ORs were 1.32 (0.85, 2.06) and 1.00 (0.68, 1.48). The ORs for prevalent RA among participants missing 5-8, 9-14, 15-31 or 32 teeth (versus 0-4 teeth) were 1.74 (1.03, 2.95), 1.82 (0.81, 4.10), 1.45 (0.62, 3.41) and 1.30 (0.48, 3.53); ORs for incident RA were 1.12 (0.77, 1.64), 1.67 (1.12, 2.48), 1.40 (0.85, 2.33) and 1.22 (0.75, 2.00). Dose-responsiveness was enhanced among never smokers. The rate of death or loss-to-follow-up after 1982 was two- to fourfold higher among participants with periodontitis or missing ≥9 teeth (versus healthy participants).
Conclusions: Although participants with periodontal disease or ≥5 missing teeth experienced higher odds of prevalent/incident RA, most ORs were non-statistically significant and lacked dose-responsiveness. Differential RA ascertainment bias complicated the interpretation of these data.
© 2011 John Wiley & Sons A/S.
Figures
References
-
- AL-KATMA MK, BISSADA NF, BORDEAUX JM, SUE J, ASKARI AD. Control of periodontal infection reduces the severity of active rheumatoid arthritis. J Clin Rheumatol. 2007;13:134–7. - PubMed
-
- ARNETT FC, EDWORTHY SM, BLOCH DA, MCSHANE DJ, FRIES JF, COOPER NS, HEALEY LA, KAPLAN SR, LIANG MH, LUTHRA HS, MEDSGER TA, MITCHELL DM, NEUSTADT DH, PINALS RS, SCHALLER JG, SHARP JT, WILDER RL, HUNDER GG. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31:315–24. - PubMed
-
- BARTOLD PM, MARINO V, CANTLEY M, HAYNES DR. Effect of Porphyromonas gingivalis-induced inflammation on the development of rheumatoid arthritis. Journal of Clinical Periodontology. 2010;37:405–11. - PubMed
-
- CANTLEY MD, HAYNES DR, MARINO V, BARTOLD PM. Pre-existing periodontitis exacerbates experimental arthritis in a mouse model. Journal of Clinical Periodontology. 2011;38:532–41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
