

Cardiovascular dysautonomia in Parkinson disease: from pathophysiology to pathogenesis
- PMID: 22094370
- PMCID: PMC3299874
- DOI: 10.1016/j.nbd.2011.10.025
Cardiovascular dysautonomia in Parkinson disease: from pathophysiology to pathogenesis
Abstract
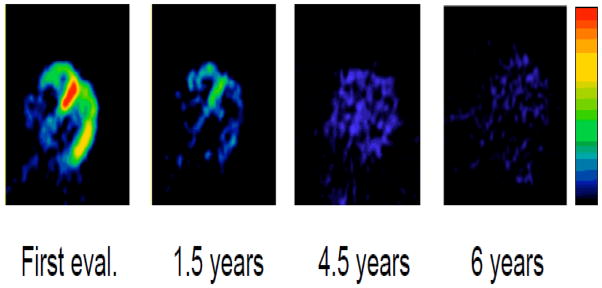
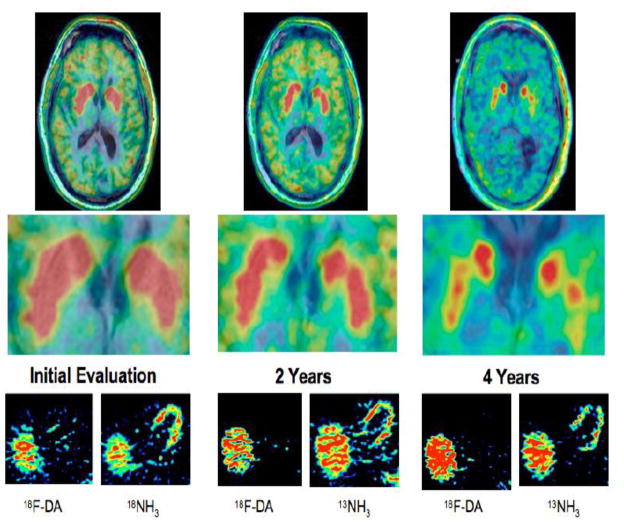
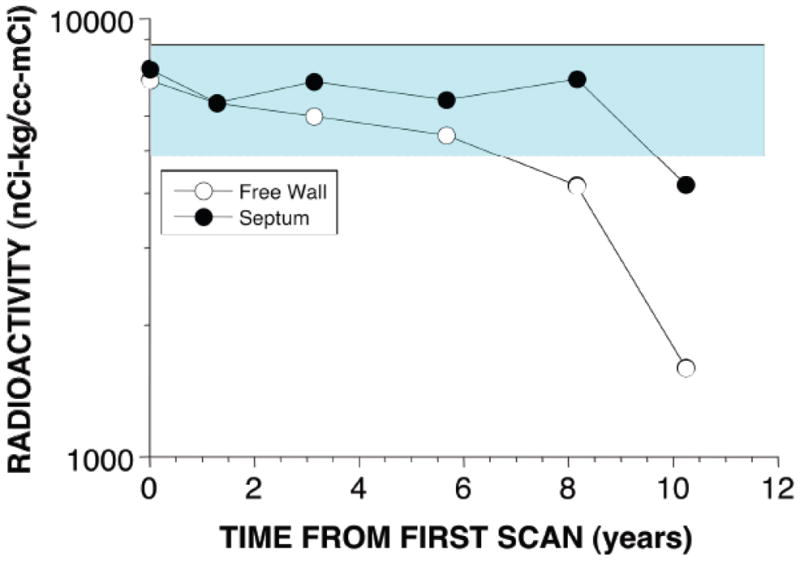
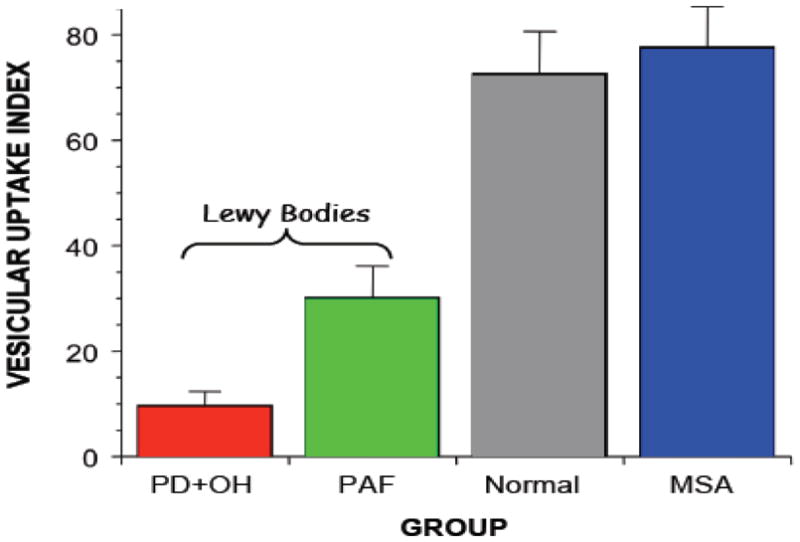
Signs or symptoms of impaired autonomic regulation of circulation often attend Parkinson disease (PD). This review covers biomarkers and mechanisms of autonomic cardiovascular abnormalities in PD and related alpha-synucleinopathies. The clearest clinical laboratory correlate of dysautonomia in PD is loss of myocardial noradrenergic innervation, detected by cardiac sympathetic neuroimaging. About 30-40% of PD patients have orthostatic hypotension (OH), defined as a persistent, consistent fall in systolic blood pressure of at least 20 mmHg or diastolic blood pressure of at least 10 mmHg within 3 min of change in position from supine to standing. Neuroimaging evidence of cardiac sympathetic denervation is universal in PD with OH (PD+OH). In PD without OH about half the patients have diffuse left ventricular myocardial sympathetic denervation, a substantial minority have partial denervation confined to the inferolateral or apical walls, and a small number have normal innervation. Among patients with partial denervation the neuronal loss invariably progresses over time, and in those with normal innervation at least some loss eventually becomes evident. Thus, cardiac sympathetic denervation in PD occurs independently of the movement disorder. PD+OH also entails extra-cardiac noradrenergic denervation, but this is not as severe as in pure autonomic failure. PD+OH patients have failure of both the parasympathetic and sympathetic components of the arterial baroreflex. OH in PD therefore seems to reflect a "triple whammy" of cardiac and extra-cardiac noradrenergic denervation and baroreflex failure. In contrast, most patients with multiple system atrophy, which can resemble PD+OH clinically, do not have evidence for cardiac or extra-cardiac noradrenergic denervation. Catecholamines in the neuronal cytoplasm are potentially toxic, via spontaneous and enzyme-catalyzed oxidation. Normally cytoplasmic catecholamines are efficiently taken up into vesicles via the vesicular monoamine transporter. The recent finding of decreased vesicular uptake in Lewy body diseases therefore suggests a pathogenetic mechanism for loss of catecholaminergic neurons in the periphery and brain. Parkinson disease (PD) is one of the most common chronic neurodegenerative diseases of the elderly, and it is likely that as populations age PD will become even more prevalent and more of a public health burden. Severe depletion of dopaminergic neurons of the nigrostriatal system characterizes and likely produces the movement disorder (rest tremor, slowness of movement, rigid muscle tone, and postural instability) in PD. Over the past two decades, compelling evidence has accrued that PD also involves loss of noradrenergic neurons in the heart. This finding supports the view that loss of catecholaminergic neurons, both in the nigrostriatal system and the heart, is fundamental in PD. By the time PD manifests clinically, most of the nigrostriatal dopaminergic neurons are already lost. Identifying laboratory measures-biomarkers-of the disease process is therefore crucial for advances in treatment and prevention. Deposition of the protein, alpha-synuclein, in the form of Lewy bodies in catecholaminergic neurons is a pathologic hallmark of PD. Alpha-synucleinopathy in autonomic neurons may occur early in the pathogenetic process. The timing of cardiac noradrenergic denervation in PD is therefore a key issue. This review updates the field of autonomic cardiovascular abnormalities in PD and related disorders, with emphasis on relationships among striatal dopamine depletion, sympathetic noradrenergic denervation, and alpha-synucleinopathy.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
References
-
- Braak H, et al. Stages in the development of Parkinson's disease-related pathology. Cell Tissue Res. 2004;318:121–134. - PubMed
-
- Braak H, et al. Idiopathic Parkinson's disease: possible routes by which vulnerable neuronal types may be subject to neuroinvasion by an unknown pathogen. J Neural Transm. 2003;110:517–36. - PubMed
-
- Burke WJ, et al. Aggregation of alpha-synuclein by DOPAL, the monoamine oxidase metabolite of dopamine. Acta Neuropathol. 2008;115:193–203. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
