

A method to estimate the chronic health impact of air pollutants in U.S. residences
- PMID: 22094717
- PMCID: PMC3279453
- DOI: 10.1289/ehp.1104035
A method to estimate the chronic health impact of air pollutants in U.S. residences
Abstract
Background: Indoor air pollutants (IAPs) cause multiple health impacts. Prioritizing mitigation options that differentially affect individual pollutants and comparing IAPs with other environmental health hazards require a common metric of harm.
Objectives: Our objective was to demonstrate a methodology to quantify and compare health impacts from IAPs. The methodology is needed to assess population health impacts of large-scale initiatives-including energy efficiency upgrades and ventilation standards-that affect indoor air quality (IAQ).
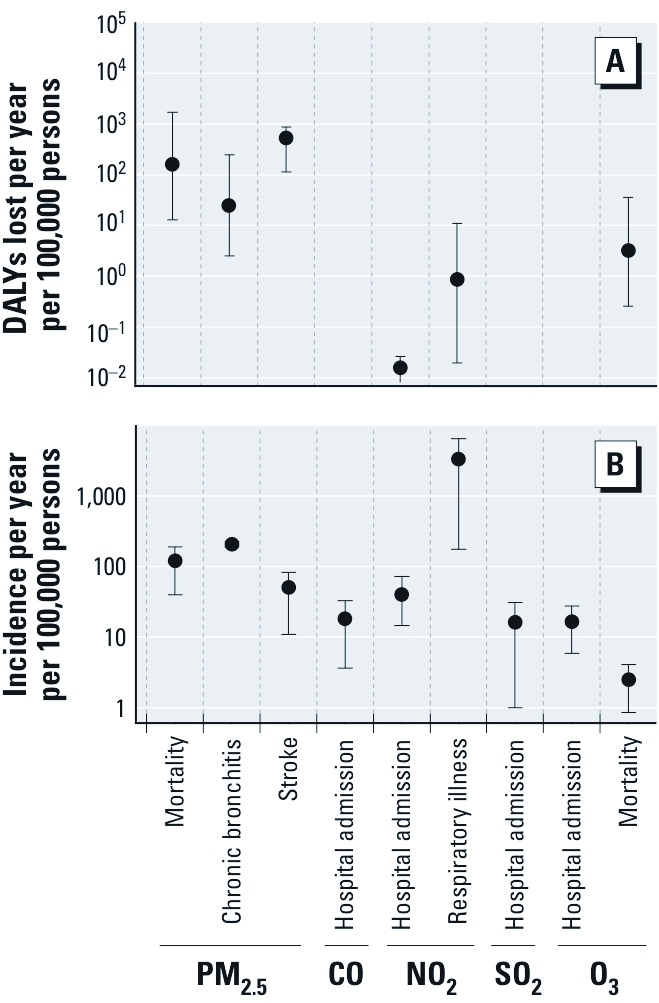
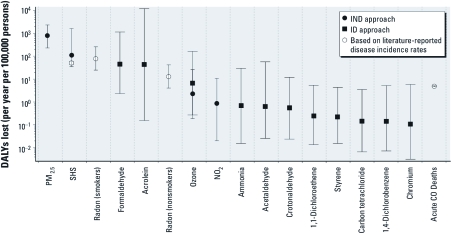
Methods: Available disease incidence and disease impact models for specific pollutant-disease combinations were synthesized with data on measured concentrations to estimate the chronic heath impact, in disability-adjusted life-years (DALYs) lost, due to inhalation of a subset of IAPs in U.S. residences. Model results were compared with independent estimates of DALYs lost due to disease.
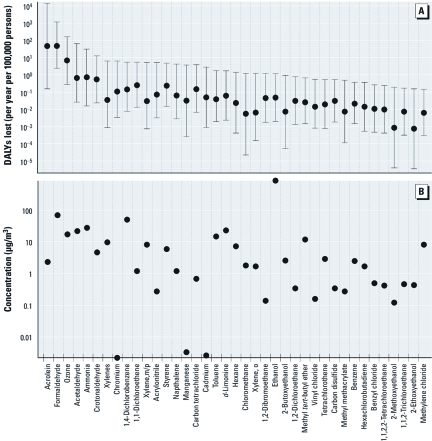
Results: Particulate matter ≤ 2.5 μm in aerodynamic diameter (PM2.5), acrolein, and formaldehyde accounted for the vast majority of DALY losses caused by IAPs considered in this analysis, with impacts on par or greater than estimates for secondhand tobacco smoke and radon. Confidence intervals of DALYs lost derived from epidemiology-based response functions are tighter than those derived from toxicology-based, interspecies extrapolations. Statistics on disease incidence in the United States indicate that the upper-bound confidence interval for aggregate IAP harm is implausibly high.
Conclusions: The approach demonstrated in this study may be used to assess regional and national initiatives that affect IAQ at the population level. Cumulative health impacts from inhalation in U.S. residences of the IAPs assessed in this study are estimated at 400-1,100 DALYs lost annually per 100,000 persons.
Conflict of interest statement
The authors declare they have no actual or potential competing financial interests.
Figures
References
-
- Abbey DE, Ostro BE, Petersen F, Burchette RJ. Chronic respiratory symptoms associated with estimated long-term ambient concentrations of fine particulates less than 2.5 microns in aerodynamic diameter (PM2.5) and other air pollutants. J Expo Anal Environ Epidemiol. 1995;5(2):137–159. - PubMed
-
- Brook RD, Rajagopalan S, Pope CA, III, Brook JR, Bhatnagar A, Diez-Roux AV, et al. Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation. 2010;121(21):2331–2378. - PubMed
-
- Burnett RT, Smith-Doiron D, Stieb D, Cakmak S, Brook JR. Effects of particulate and gaseous air pollution on cardiorespiratory hospitalizations. Arch Environ Health. 1999;54(2):130–139. - PubMed
-
- CAAA (Clean Air Act Amendments of 1970) 1970. Pub. L. No. 91-604, 84 Stat. 1676 (codified as amended in scattered sections of 42 U.S.C.).
-
- CAAA (Clean Air Act Amendments of 1990) 1990. Pub. L. No. 101-549, 104 Stat. 2399 (codified as amended in scattered sections of 42 U.S.C.).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
