

Solitary rectal ulcer syndrome in children and adolescents
- PMID: 22094902
- PMCID: PMC3719860
- DOI: 10.1097/MPG.0b013e318240bba5
Solitary rectal ulcer syndrome in children and adolescents
Abstract
Objectives: The aim of this study was to describe the presenting symptoms, endoscopic and histologic findings, and clinical courses of pediatric patients diagnosed with solitary rectal ulcer syndrome (SRUS).
Methods: We describe 15 cases of SRUS diagnosed at our institution during a 13-year period. Cases were identified by review of a pathology database and chart review and confirmed by review of biopsies. Data were collected by retrospective chart review.
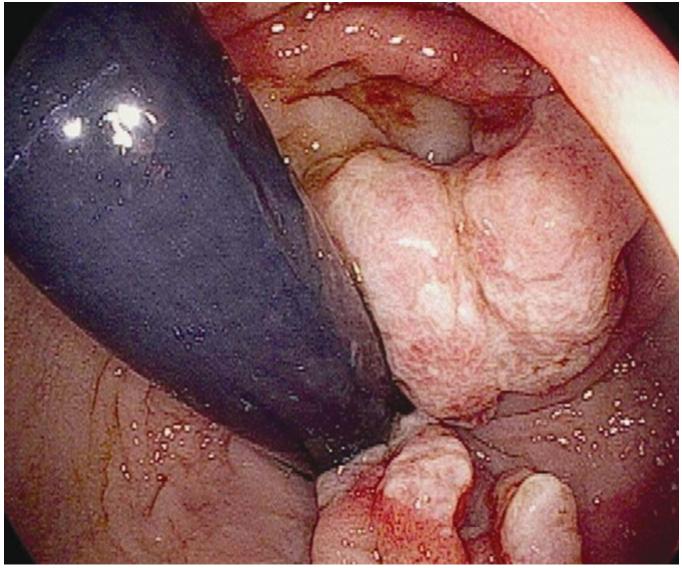
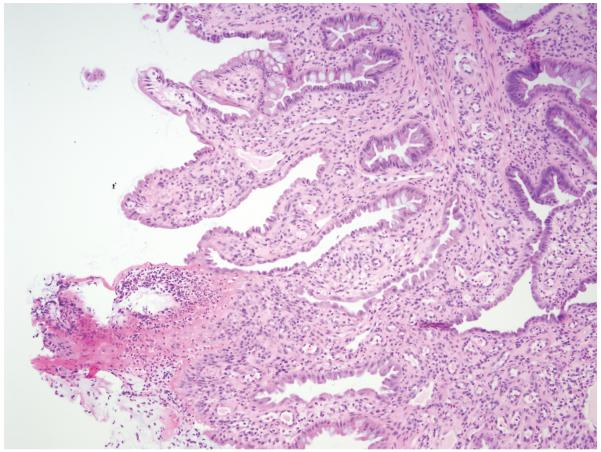
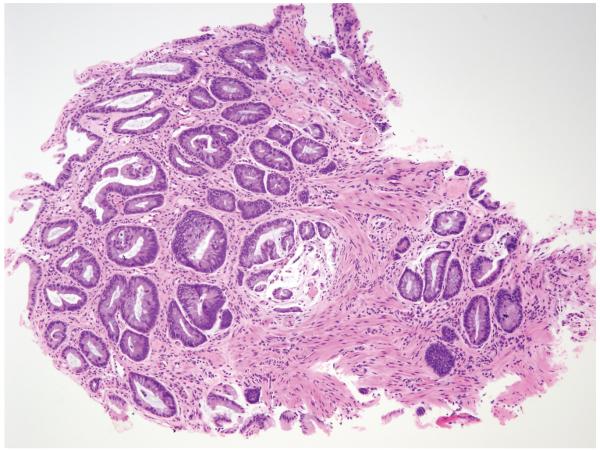
Results: Presenting symptoms were consistent but nonspecific, most commonly including blood in stools, diarrhea alternating with constipation, and abdominal/perianal pain. Fourteen of 15 patients had normal hemoglobin/hematocrit, erythrocyte sedimentation rate, and albumin at diagnosis. Endoscopic findings, all limited to the distal rectum, ranged from erythema to ulceration and polypoid lesions. Histology revealed characteristic findings. Stool softeners and mesalamine suppositories improved symptoms, but relapse was common.
Conclusions: SRUS in children presents with nonspecific symptoms and endoscopic findings. Clinical suspicion is required, and diagnosis requires histologic confirmation. Response to present treatments is variable.
Figures
Comment in
-
An overlooked entity in children with rectal bleeding: solitary rectal ulcer.J Pediatr Gastroenterol Nutr. 2012 Feb;54(2):169-70. doi: 10.1097/MPG.0b013e318240bbc2. J Pediatr Gastroenterol Nutr. 2012. PMID: 22094903 No abstract available.
References
-
- Keshtgar AS. Solitary rectal ulcer syndrome in children. Eur J Gastroenterol Hepatol. 2008:89–92. - PubMed
-
- De la Rubia L, Ruiz Villaespesa A, Cebrero M, et al. Solitary rectal ulcer syndrome in a child. J Pediatr. 1993:733–6. - PubMed
-
- Dehghani SM, Haghighat M, Imanieh MH, et al. Solitary rectal ulcer syndrome in children: A prospective study of cases from southern iran. Eur J Gastroenterol Hepatol. 2008:93–5. - PubMed
-
- Ertem D, Acar Y, Karaa EK, et al. A rare and often unrecognized cause of hematochezia and tenesmus in childhood: Solitary rectal ulcer syndrome. Pediatrics. 2002:e79. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
