

Personalizing medicine with clinical pharmacogenetics
- PMID: 22095251
- PMCID: PMC3290900
- DOI: 10.1097/GIM.0b013e318238b38c
Personalizing medicine with clinical pharmacogenetics
Abstract
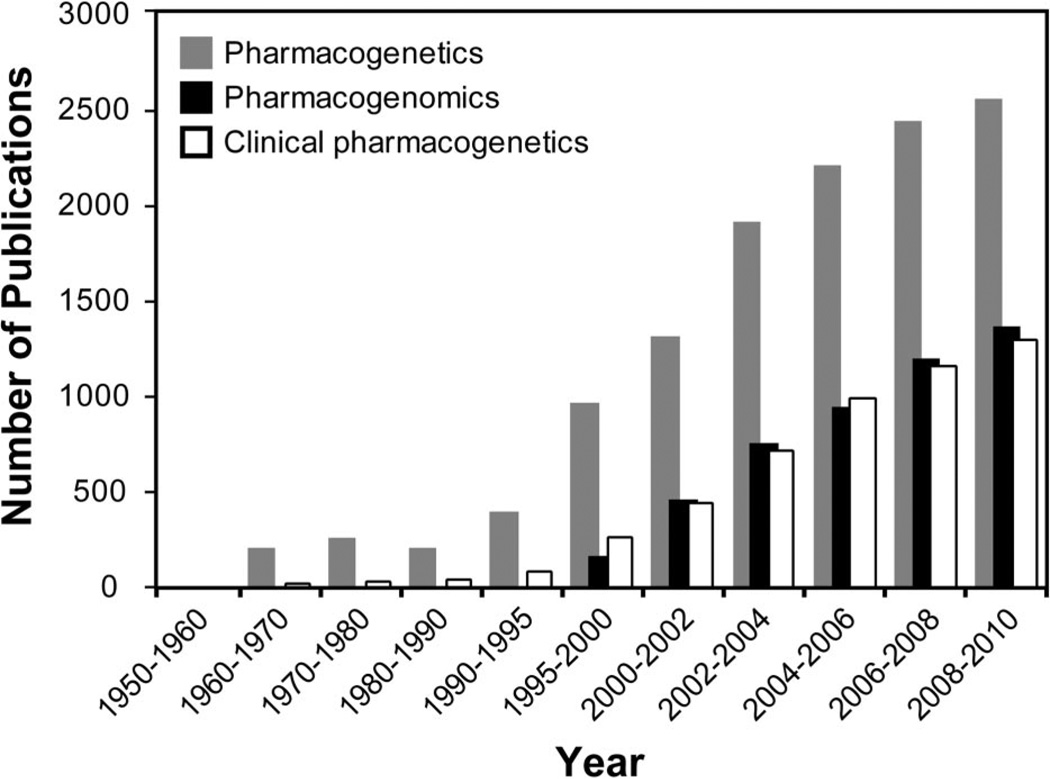
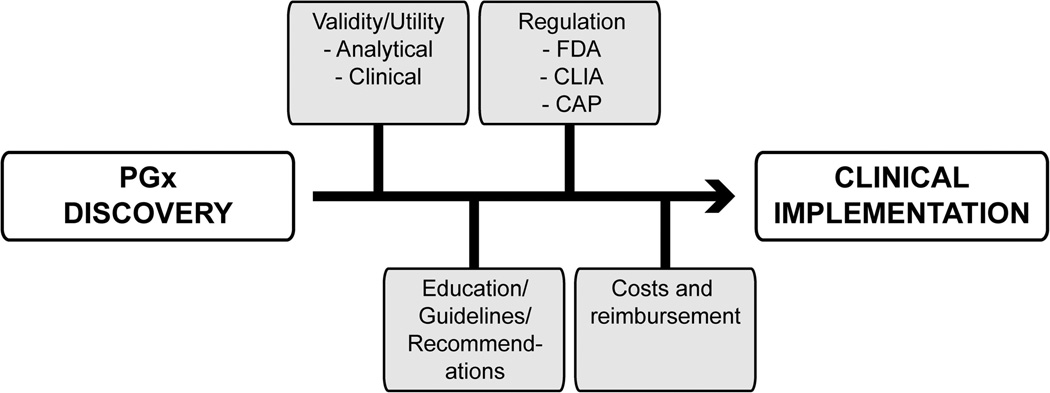
Clinical genetic testing has grown substantially over the past 30 years as the causative mutations for Mendelian diseases have been identified, particularly aided in part by the recent advances in molecular-based technologies. Importantly, the adoption of new tests and testing strategies (e.g., diagnostic confirmation, prenatal testing, and population-based carrier screening) has often been met with caution and careful consideration before clinical implementation, which facilitates the appropriate use of new genetic tests. Although the field of pharmacogenetics was established in the 1950s, clinical testing for constitutional pharmacogenetic variants implicated in interindividual drug response variability has only recently become available to help clinicians guide pharmacotherapy, in part due to US Food and Drug Administration-mediated product insert revisions that include pharmacogenetic information for selected drugs. However, despite pharmacogenetic associations with adverse outcomes, physician uptake of clinical pharmacogenetic testing has been slow. Compared with testing for Mendelian diseases, pharmacogenetic testing for certain indications can have a lower positive predictive value, which is one reason for underutilization. A number of other barriers remain with implementing clinical pharmacogenetics, including clinical utility, professional education, and regulatory and reimbursement issues, among others. This review presents some of the current opportunities and challenges with implementing clinical pharmacogenetic testing.
Conflict of interest statement
Disclosure: The author declares no conflict of interest.
Figures
References
-
- Kan YW, Dozy AM. Antenatal diagnosis of sickle-cell anaemia by D.N.A. analysis of amniotic-fluid cells. Lancet. 1978;2:910–912. - PubMed
-
- Patrinos GP, Kollia P, Papadakis MN. Molecular diagnosis of inherited disorders: lessons from hemoglobinopathies. Hum Mutat. 2005;26:399–412. - PubMed
-
- Motulsky AG. Drug reactions enzymes, and biochemical genetics. J AmMed Assoc. 1957;165:835–837. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
